


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of Action/Pharmacodynamic Properties (PD): Pathological changes in dementia such as Alzheimer's Disease involve cholinergic neuronal pathways that project from the basal forebrain to the cerebral cortex and hippocampus. These pathways are known to be involved in attention, learning and memory and other cognitive processes. Rivastigmine, a brain-selective acetyl- and butyryl-cholinesterase inhibitor of the carbamate type, is thought to facilitate cholinergic neurotransmission by slowing the degradation of acetylcholine released by functionally intact cholinergic neurons. Data from animal studies indicate that rivastigmine selectively increases the availability of acetylcholine in the cortex and hippocampus. Thus, Exelon may have an ameliorative effect on cholinergic-mediated cognitive deficits associated with Alzheimer's Disease and with Parkinson's disease. In addition, there is some evidence that cholinesterase inhibition could slow the formation of amyloidogenic beta-amyloid-precursor protein (APP) fragments, and thus of amyloid plaques, which are one of the main pathological features of Alzheimer's Disease.
Rivastigmine interacts with its target enzymes by forming a covalently bound complex that temporarily inactivates the enzymes. In healthy young men, an oral 3.0 mg dose decreases acetylcholinesterase (AChE) activity in cerebro spinal fluid (CSF) by approximately 40% within the first 1.5 hours after administration. Activity of the enzyme returns to baseline levels about 9 hours after the maximum inhibitory effect has been achieved. Butyrylcholinesterase (BuChE) activity in CSF was transiently inhibited and was no longer different from baseline after 3.6 hours in healthy young volunteers. In patients with Alzheimer's Disease (AD), inhibition of acetylcholinesterase in CSF by rivastigmine was dose-dependent up to 6 mg given twice daily, the highest dose tested. Inhibition of BuChE activity in CSF of AD patients by rivastigmine was similar to that of AchE, with a change from baseline of more than 60% after 6 mg given twice daily. The effect of rivastigmine on AChE and BuChE activity in CSF was sustained after 12 months administration, the longest time studied. Statistically significant correlations were found between the degree of inhibition by rivastigmine of AChE and BuChE in the CSF and changes on a compound measure of cognitive performance in AD patients; however, only BuChE inhibition in CSF was significantly and consistently correlated with improvements in speed-, attention- and memory-related subtests.
Clinical Studies: Clinical studies in Alzheimer's Dementia: The efficacy of Exelon in the treatment of Alzheimer's Disease has been demonstrated in placebo-controlled studies. The patients involved had an MMSE (Mini-Mental State Examination) of 10-24. Results from two pivotal 26-week multicentre studies comparing 1-4 mg/day and 6-12 mg/day with placebo, as well as pooled analysis of Phase III studies have established that Exelon produces significant improvement in the major domains of cognition, global functioning and activities of daily living, and in disease severity. Both the low and high dose ranges showed benefit for cognition, global functioning, and disease severity; in addition, the higher dose range produced benefit in activities of daily living.
The following key outcome measures were used in these studies: Alzheimer's Disease Assessment Scale (ADAS-Cog): A performance-based test system that measures cognitive areas relevant for patients with Alzheimer's Disease such as attention, learning, memory and language.
Clinician Interview Based Impression of Change-Plus (CIBIC-Plus): A clinician-rated assessment of the patient's global change in the domains of cognition, behaviour and functioning, incorporating separate patient and caregiver inputs.
Progressive Deterioration Scale (PDS): A caregiver-rated evaluation of the patient's ability to perform activities of daily living such as toileting, washing, eating, and helping with household chores and shopping.
Study results have indicated that onset of efficacy is generally as early as week 12 and is maintained at the end of 6 months of treatment. Patients treated with 6-12 mg experienced improvement in cognition, activities of daily living and global functioning, while placebo patients showed deterioration. The effects of Exelon on these measures (e.g. ADAS-Cog difference from placebo 5 points at week 26) indicate a delay in the rate of deterioration of at least 6 months.
Analyses performed to detect those subtests and symptoms of the ADAS-Cog and CIBIC-Plus, respectively, which improved in patients treated with Exelon indicated that all ADAS-Cog subtests (ideational praxis, orientation, test instructions, word recall, language ability and word recognition) and all CIBIC-Plus items, except anxiety, were significantly improved at week 26 with Exelon 6-12 mg. Items which improved in at least 15% more Exelon than placebo patients completing treatment included word recall, functioning, agitation, tearfulness or crying, delusions, hallucinations, purposeless and inappropriate activities, and physical threats and/or violence.
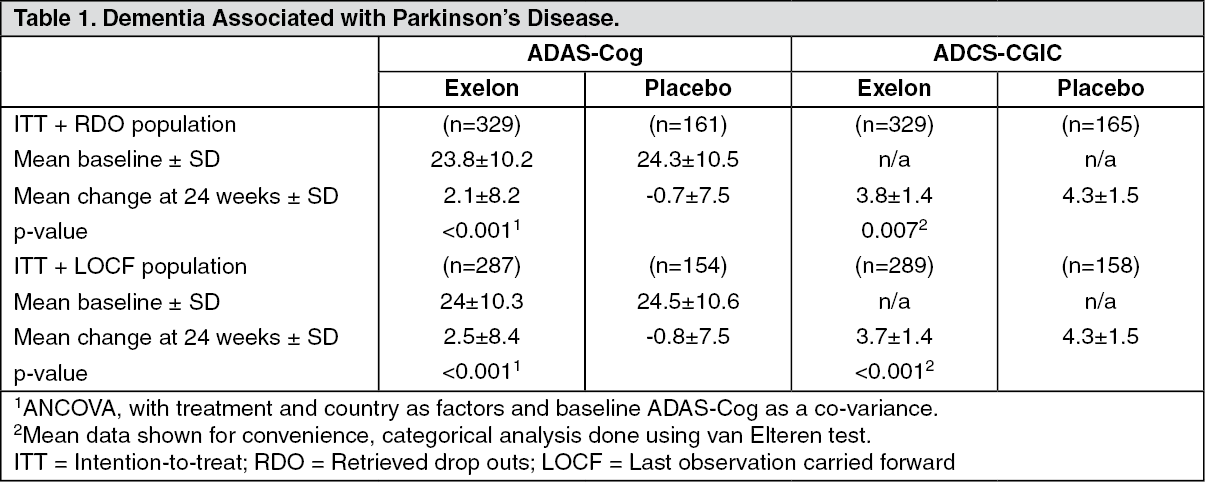
Clinical studies in dementia associated with Parkinson's disease: The efficacy of rivastigmine in dementia associated with Parkinson's disease has been demonstrated in a 24-week multicentre, double blind, placebo-controlled core study and its 24-week open-label extension phase. Patients involved in this study had an MMSE (Mini-Mental State Examination) of 10-24. Efficacy has been established by the use of two independent scales which were assessed at regular intervals during a 6-month treatment period as reported in Table 1: the ADAS-cog, a measure of cognition and the global measure ADCS-CGIC (Alzheimer's Disease Cooperative Study-Clinician's Global Impression of Change). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: Rivastigmine is rapidly and completely absorbed. Peak plasma concentrations are reached in approximately 1 hour. As a consequence of the drug's interaction with its target enzyme, the increase in bioavailability is about 1.5-fold greater than that expected from the increase in dose. Absolute bioavailability after a 3 mg dose is about 36%. Administration of rivastigmine capsules with food delays absorption (tmax) by 90 min and lowers Cmax and increases AUC by approximately 30%.
Distribution: Rivastigmine is weakly bound to plasma proteins (approximately 40%). Rivastigmine distributes equally between blood and plasma with a blood-to-plasma partition ratio of 0.9 at concentrations ranging from 1 to 400 ng/mL. It readily crosses the blood brain barrier reaching peak concentrations in 1 to 4 hours, and with a cerebrospinal fluid-to-plasma AUC ratio of 40%. Rivastigmine has a volume of distribution after IV dosing in the range of 1.8-2.7 L/kg.
Metabolism: Rivastigmine is rapidly and extensively metabolised (half-life in plasma approximately 1 hour), primarily via cholinesterase-mediated hydrolysis to the decarbamylated metabolite. In vitro, this metabolite shows minimal inhibition of acetylcholinesterase (<10%). Based on in vitro studies, no pharmacokinetic drug interactions are expected with drugs metabolized by the following cytochrome isoenzymes: CYP1A2, CYP2D6, CYP3A4/5, CYP2E1, CYP2C9, CYP2C8, CYP2C19, or CYP2B6. Based on evidence from animal studies, the major cytochrome P450 isoenzymes are minimally involved in rivastigmine metabolism. Consistent with these observations is the finding that no drug interactions relating to cytochrome P450 have been observed in humans (see Interactions).
Elimination: Unchanged rivastigmine is not found in the urine; renal excretion of the metabolites is the major route of elimination. Following administration of 14C-rivastigmine, renal elimination was rapid and essentially complete (>90%) within 24 hours. Less than 1% of the administered dose is excreted in the faeces. There is no accumulation of rivastigmine or the decarbamylated metabolite in patients with Alzheimer's Disease.
Special Population: Elderly subjects: In a study to assess the effect of age on the pharmacokinetics of 1 and 2.5 mg oral rivastigmine, plasma concentrations of rivastigmine tended to be higher in the elderly (n=24, aged 61-71 years) as compared to young subjects (n=24, aged 19-40 years) after the 1 mg dose. This difference was more pronounced with the higher dose (2.5 mg) at which rivastigmine plasma concentrations were 30% greater in the healthy elderly than in healthy young subjects. Plasma levels of the decarbamylated phenolic metabolite were not substantially affected by age. Studies in Alzheimer patients aged between 50 and 92 years, however showed no change in rivastigmine bioavailability with age.
Renal impairment: Plasma levels of rivastigmine were reported not to differ significantly between patients with severe renal impairment (n=10, glomerular filtration rate (GFR) <10 mL/minute) and control subjects (n=10, GFR ≥60 mL/min) given a single oral dose of 3 mg. Clearance of rivastigmine was 4.8 L/min and 6.9 L/min in patients and healthy subjects, respectively. However, in moderately impaired renal patients (n=8, GFR=10-50 mL/min), peak plasma concentrations of rivastigmine were increased by almost 2.5 fold and overall plasma levels (AUC) of the decarbamylated phenolic metabolite were increased by approximately 50%. Clearance of rivastigmine was 1.7 L/min. The reason for this discrepancy between severely and moderately impaired renal patients is unclear (see Dosage & Administration and Precautions).
Hepatic impairment: After oral administration, the Cmax of rivastigmine was approximately 60% higher and the AUC more than twice as high in subjects with mild to moderate hepatic impairment compared to healthy subjects. Following a single 3-mg dose or multiple 6-mg twice a day doses, the mean oral clearance of rivastigmine was approximately 60-65% lower in mild (n=7, Child-Pugh score 5-6) and moderate (n=3, Child-Pugh score 7-9) hepatically impaired patients (n=10, biopsy proven) than in healthy subjects (n=10). These pharmacokinetic changes had no effect on either the incidence or severity of adverse effects (see Dosage & Administration and Precautions).
Toxicology: Non-Clinical Safety Data: Acute toxicity: The estimated oral LD50 values in mice were 5.6 mg base/kg (males) and 13.8 mg base/kg (females). The estimated oral LD50 values in rats were 8.1 mg base/kg (males) and 13.8 mg base/kg (females).
Repeated dose toxicity: Studies in rats, mice, dogs, minipigs and monkeys (maximum doses 3.8, 6.3, 2.5, 6.0 and 6.3 mg-base/kg/day, respectively) revealed evidence of cholinergic stimulation of the central and peripheral nervous systems. In-life tolerability to rivastigmine was variable between species, with the dog as the most sensitive species. No target organ toxicities or clinical pathology alterations were observed in any species, although gastro-intestinal effects were prominent in dogs.
Mutagenicity: Rivastigmine was not mutagenic in in vitro tests for gene mutations and primary DNA damage. In tests for chromosomal damage in vitro, a small increase in the number of cells carrying chromosomal aberrations occurred at very high concentrations. However, as there was no evidence of clastogenic activity in the more relevant in vivo micronucleus test assessing chromosomal damage, it is most likely that the in vitro findings were false positive observations.
Carcinogenicity: No evidence of carcinogenicity was found in oral and topical studies in mice and in oral study in rats at the maximum tolerated dose. The exposure to rivastigmine and its major metabolite was approximately equivalent to human exposure with highest doses of rivastigmine capsules and patches.
Reproductive toxicity: Oral studies in pregnant rats and rabbits with dose levels up to 2.3 mg base/kg/day gave no indication of teratogenic potential on the part of rivastigmine. Similarly, there was no evidence of adverse effects of rivastigmine on fertility, reproductive performance or in utero or postnatal growth and development in rats at given dose levels up to 1.1 mg base/kg/day (see Use in Pregnancy & Lactation).