


 Sign Out
Sign Out

Rilpivirine activity is mediated by non-competitive inhibition of HIV-1 reverse transcriptase (RT).
Rilpivirine does not inhibit the human cellular DNA polymerases α, β and γ.
Pharmacodynamics: Effect on Electrocardiogram: The effect of EDURANT on the QTc interval of the ECG was evaluated in two Phase I studies in healthy adult volunteers. EDURANT at the recommended therapeutic dose of 25 mg q.d. was examined in a double-blind, double-dummy, randomized, placebo- and active-controlled, three-way crossover study in healthy adult volunteers (N=60, 35M/25F), with 13 ECG recordings over 24 hours on day 11 of treatment (steady-state). EDURANT at the dose of 25 mg q.d. was not associated with a statistically significant or clinically relevant effect on the QTc interval. EDURANT at doses of 75 mg q.d., and 300 mg q.d. was studied in a double-blind, double-dummy, randomized, placebo and active controlled, three-way crossover study in healthy adult volunteers (N=41, 22F/19M), with 13 ECG recordings over 24 hours on day 1 and day 11 of treatment. On day 11 of treatment (steady-state), the maximum mean QTc interval prolongation (baseline- and placebo-adjusted) was 10.7 (90% CI 6.1, 15.3) ms in the 75 mg q.d. treatment arm and 23.3 (90% CI 18.0, 28.7) ms at 4.5 h post-dosing in the 300 mg q.d. arm.
For QTc interval effects with long-term treatment in the target patient population see Abnormal Laboratory Findings: Hematologic, Clinical Chemistry and Other Quantitative Data: Electrocardiogram Findings under Adverse Reactions. See also Cardiovascular under Precautions and QT Prolonging Drugs under Interactions.
Safety Pharmacology: Concentration-dependent inhibition of potassium-currents involved in the repolarisation of the cardiac action potential and prolongation of QT interval from baseline in arterially perfused rabbit left ventricular wedge preparations were observed in the in vitro safety pharmacology studies.
In an antibody-based chemoluminescent assay, rilpivirine was found to decrease the surface expression of hERG potassium channels by 29% and 36% at nominal concentrations of 3.7 and 11.0 μg/mL.
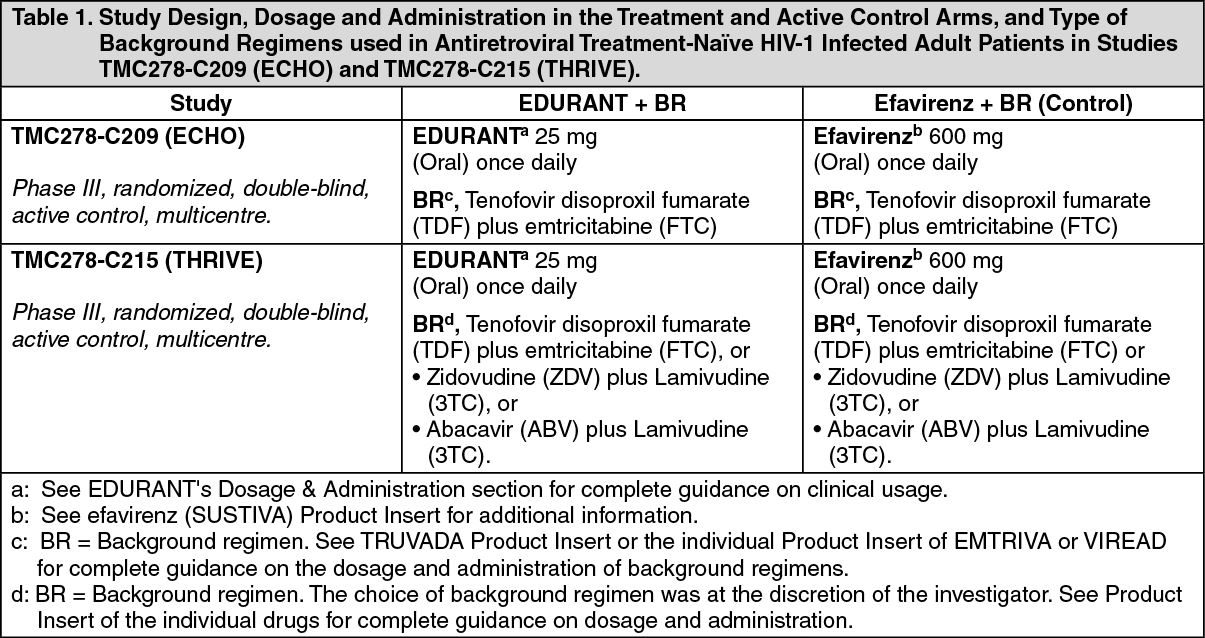
Clinical Trials: Trial Design and Study Demographics: Treatment-Naïve Adult Patients: Trial TMC278-C209 (ECHO) and TMC278-C215 (THRIVE): The evidence of efficacy of EDURANT (rilpivirine) is based on the analyses of 48 and 96-week data from two Phase III trials in antiretroviral treatment-naïve HIV-1 infected adult subjects (Table 1). Similar efficacy for EDURANT was seen in each trial demonstrating non-inferiority to efavirenz.
Subjects with plasma HIV-1 RNA ≥5000 copies/mL, who were screened for susceptibility to N(t)RTIs and for absence of specific NNRTI RAMs, were included in the trials. The treatments are summarized in Table 1: See Table 1.
 Click on icon to see table/diagram/image
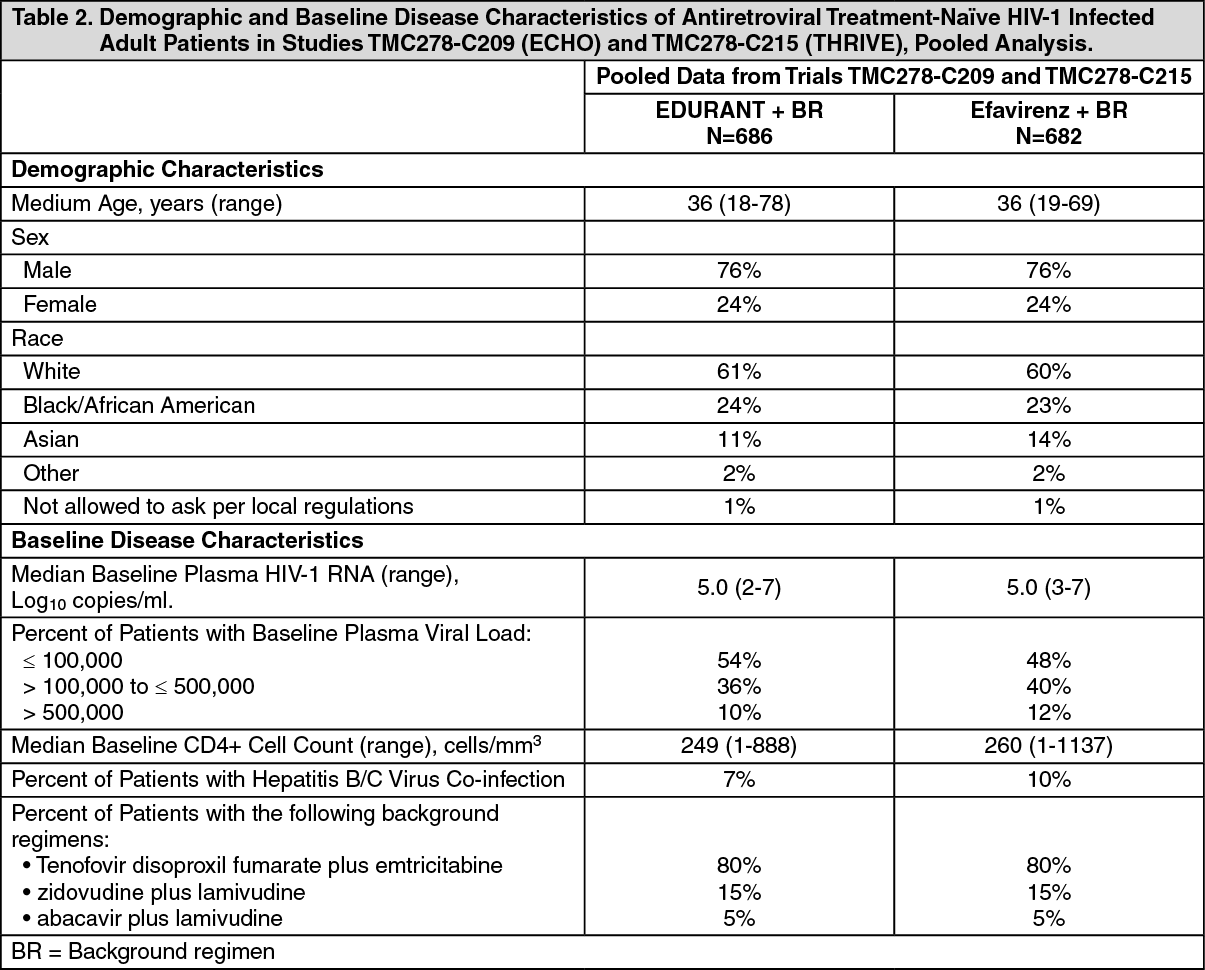
Click on icon to see table/diagram/imageIn the pooled analyses of TMC278-C209 and TMC278-C215 the demographic and baseline disease characteristics were balanced between the EDURANT arm and efavirenz (control) arms (Table 2). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageStudy Results: Efficacy at Week 48 and Week 96 for subjects in the EDURANT and efavirenz arms for the pooled data from the TMC278-C209 and TMC278-C215 study populations are shown in Table 3. The response rate (confirmed undetectable viral load < 50 HIV-1 RNA copies/mL) at Week 96 was comparable between the EDURANT arm and the efavirenz arm. The incidence of virologic failure was higher in the EDURANT arm than the efavirenz arm at Week 96; however, most of the virologic failures occurred within the first 48 weeks of treatment. Discontinuations due to adverse events were higher in the efavirenz arm than the EDURANT arm. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAt week 48, the mean change from baseline in CD4+ cell count was 192 cells/mm3 in the EDURANT-treated subjects and 176 cells/mm3 in the efavirenz-treated subjects in the pooled analysis of the ECHO and THRIVE trials [estimated treatment difference (95% CI): 18.0 (2.2; 33.7)].
At week 96, the mean change from baseline in CD4+ cell count was 228 cells/mm3 in the EDURANT-treated subjects and 219 cells/mm3 in the efavirenz-treated subjects [estimated treatment difference (95% CI): 11.3 (-6.8; 29.4)].
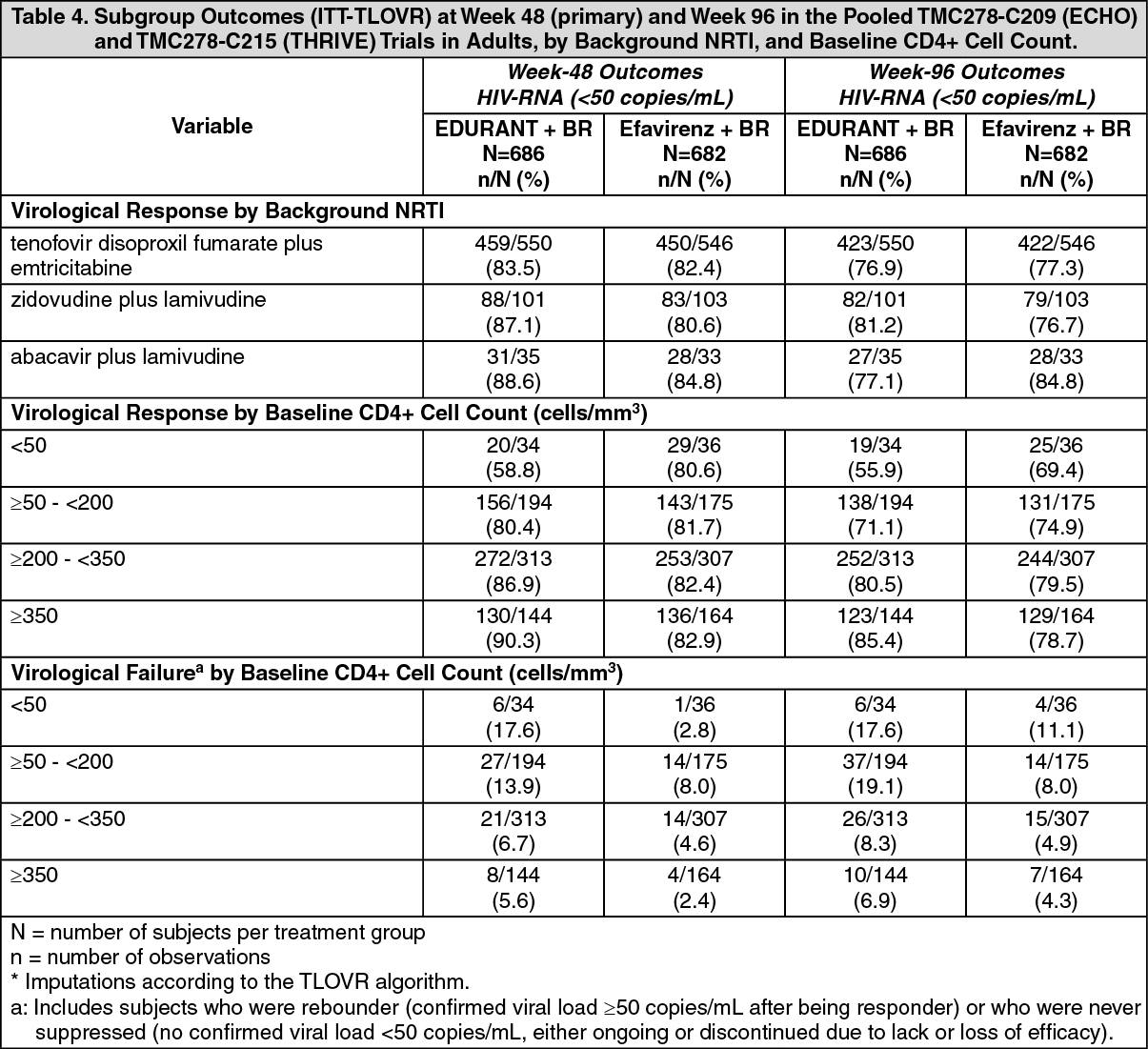
A subgroup analysis of the virological response (<50 HIV-1 RNA copies/mL, TLOVR) at 48 and 96 weeks by background NRTIs, and by CD4+ cell count, and virological failure by CD4+ cell count (pooled data from the TMC278-C209 and TMC278-C215 trials) is presented in Table 4. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTrial TMC278-C204: Study TMC278-C204 was a randomized, active-controlled, Phase IIb trial in antiretroviral treatment-naïve HIV-1-infected adult subjects consisting of 2 parts: an initial 96 weeks, partially-blinded dose-finding part (EDURANT doses blinded) followed by a long-term, open-label part. After Week 96, subjects randomized to one of the 3 doses of EDURANT were switched to EDURANT 25 mg once daily. Subjects in the control arm received efavirenz 600 mg once daily in addition to a BR in both parts of the study. The BR consisted of 2 investigator-selected N(t)RTIs: zidovudine plus lamivudine or tenofovir disoproxil fumarate plus emtricitabine.
Study TMC278-C204 enrolled 368 HIV-1-infected treatment-naïve adult subjects who had a plasma HIV-1 RNA ≥5000 copies/ml, previously received ≤2 weeks of treatment with an N(t)RTI or protease inhibitor, had no prior use of NNRTIs, and were screened for susceptibility to N(t)RTI and for absence of specific NNRTI RAMs.
At 96 weeks, the proportion of subjects with <50 HIV-1 RNA copies/mL receiving EDURANT 25 mg (N = 93) compared to subjects receiving efavirenz (N = 89) was 76% and 71%, respectively. The mean increase from baseline in CD4+ counts was 146 cells/mm3 in subjects receiving EDURANT 25 mg and 160 cells/mm3 in subjects receiving efavirenz.
At 240 weeks, 60% (56/93) of subjects who originally received 25 mg once daily achieved HIV RNA <50 copies/mL compared to 57% (51/89) of subjects in the control group.
Treatment-Naïve Pediatric Patients (12 years to less than 18 years of age): Trial TMC278-C213: The pharmacokinetics, safety, tolerability and efficacy of EDURANT 25 mg once daily, in combination with an investigator-selected background regimen (BR) containing two NRTIs, was evaluated in trial TMC278-C213, a single-arm, open-label Phase II trial in antiretroviral treatment-naive HIV-1 infected pediatric subjects 12 to less than 18 years of age and weighing at least 32 kg. This analysis included 36 patients who had completed at least 48 weeks of treatment or discontinued earlier. The 36 subjects had a median age of 14.5 years (range: 12 to 17 years), and were 55.6% female, 88.9% Black and 11.1% Asian.
In the efficacy analysis, most subjects (75%; 28/36) had baseline HIV RNA <100,000 copies/mL. For these 28 subjects the median baseline plasma HIV-1 RNA was 44,250 (range: 2,060-92,600 copies/mL) and the median baseline CD4+ cell count was 445.5 cells/mm3 (range: 123 to 983 cells/mm3).
Among the subjects who had baseline HIV RNA ≤ 100,000, the proportion with HIV-1 RNA <50 copies/mL at Week 48 (TLOVR) was 79% (22/28), versus 50.0% (4/8) in those with >100,000 copies/mL. The proportion of virologic failures among subjects with a baseline viral load ≤100,000 copies/mL was 17.9% (5/28), versus 37.5% (3/8) in those with >100,000 copies/mL. One subject discontinued due to an adverse event and one subject discontinued due to reasons other than an adverse event or virological failure. At Week 48, the mean increase in CD4+ cell count from baseline was 201.2 cells/mm3.
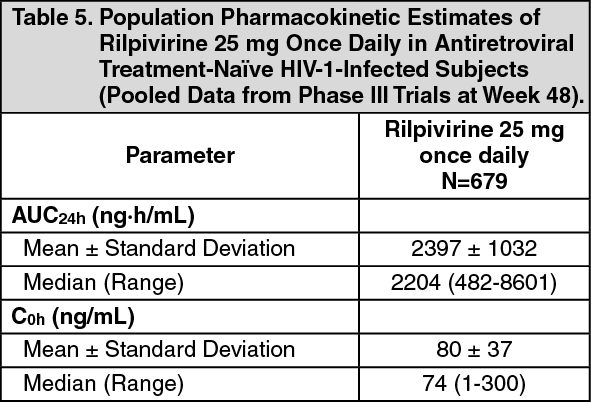
Pharmacokinetics: The pharmacokinetic properties of rilpivirine have been evaluated in adult healthy subjects and in antiretroviral treatment-naïve HIV-1-infected subjects 12 years of age and older. Exposure to rilpivirine was generally lower in HIV-1 infected subjects than in healthy subjects. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAbsorption: After oral administration, the maximum plasma concentration of rilpivirine is generally achieved within 4-5 hours. Steady-state plasma concentrations are reached in approximately 11 days. In a number of healthy subjects, multiple absorption peaks and/or an increase in absorption between 12 hours and 24 hours post-dose is observed. The underlying mechanism(s) for these observations is unknown. The absolute bioavailability of EDURANT is unknown.
Effect of food on absorption: The exposure to rilpivirine was approximately 40% lower when EDURANT was taken in a fasted condition as compared to a normal caloric meal (533 kcal) or high-fat high-caloric meal (928 kcal). When EDURANT was taken with only a protein-rich nutritional drink, exposures were 50% lower than when taken with a meal. Therefore, to achieve optimal exposure, EDURANT should be taken with a meal (see Dosage & Administration).
Distribution: Rilpivirine is approximately 99.7% bound to plasma proteins in vitro, primarily to albumin. The distribution of rilpivirine into compartments other than plasma (e.g., cerebrospinal fluid, genital tract secretions) has not been evaluated in humans.
Metabolism: In vitro experiments indicate that rilpivirine primarily undergoes oxidative metabolism mediated by the cytochrome P450 (CYP) 3A system.
Elimination: The terminal elimination half-life of rilpivirine is approximately 45 hours. After single-dose oral administration of 14C-rilpivirine, on average 85% and 6.1% of the radioactivity could be retrieved in feces and urine, respectively. In feces, unchanged rilpivirine accounted for on average 25% of the administered dose. Only trace amounts of unchanged rilpivirine (< 1% of dose) were detected in urine.
Special Populations and Conditions: Pediatrics: The pharmacokinetics of rilpivirine in antiretroviral treatment naïve HIV-1 infected pediatric subjects 12 to less than 18 years of age receiving EDURANT 25 mg once daily were comparable to those in treatment-naive HIV-1 infected adults receiving EDURANT 25 mg once daily. There was no clinically significant impact of body weight on rilpivirine pharmacokinetics in pediatric subjects in trial C213 (33 to 93 kg).
The safety and efficacy of EDURANT in pediatric patients less than 12 years of age has not been established.
Geriatrics: Clinical studies of EDURANT did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from adult subjects < 65 years of age. EDURANT should be used with caution in this population (see Use in Elderly under Precautions).
Sex: Population pharmacokinetic analysis of rilpivirine in HIV-infected patients indicated no clinically relevant differences in the pharmacokinetics of rilpivirine between men and women.
Age: Population pharmacokinetic analysis of rilpivirine in HIV-infected patients indicated no clinically relevant differences in the pharmacokinetics of rilpivirine across the age range of 18-78 years (the analysis included only two subjects above 65 years).
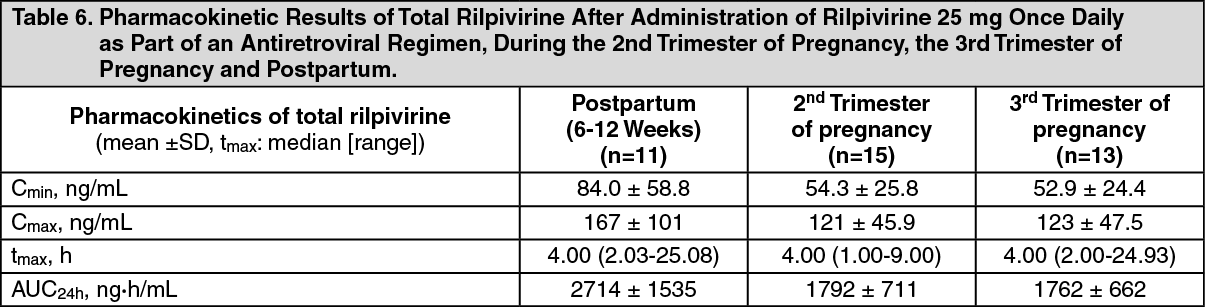
Pregnancy and Breast-feeding: Pregnancy and Postpartum: The exposure to total rilpivirine after intake of rilpivirine 25 mg once daily as part of an antiretroviral regimen was lower during pregnancy (similar for the 2nd and 3rd trimester) compared with postpartum (see Table 6). The decrease in unbound (i.e., active) rilpivirine pharmacokinetic parameters during pregnancy compared to postpartum was less pronounced than for total rilpivirine.
In women receiving rilpivirine 25 mg once daily during the 2nd trimester of pregnancy, mean intra-individual values for total rilpivirine Cmax, AUC24h and Cmin values were, respectively, 21%, 29% and 35% lower as compared to postpartum; during the 3rd trimester of pregnancy, Cmax, AUC24h and Cmin values were, respectively, 20%, 31% and 42% lower as compared to postpartum. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEthnic origin: Population pharmacokinetic analysis of rilpivirine in HIV-infected patients indicated that race had no clinically relevant effect on the pharmacokinetics of rilpivirine.
Hepatic Insufficiency: Rilpivirine is primarily metabolized and eliminated by the liver. In a study comparing 8 subjects with mild hepatic impairment (Child-Pugh score A) to 8 matched controls, and 8 subjects with moderate hepatic impairment (Child-Pugh score B) to 8 matched controls, the multiple dose exposure of rilpivirine was 47% higher in subjects with mild hepatic impairment and 5% higher in subjects with moderate hepatic impairment. EDURANT has not been studied in subjects with severe hepatic impairment (Child-Pugh score C) (see Hepatic/Biliary/Pancreatic: Hepatic Impairment under Precautions and Recommended Dose and Dosage Adjustment: Hepatic Impairment under Dosage & Administration).
Hepatitis B or Hepatitis C Virus Co-infection: Population pharmacokinetic analysis indicated that hepatitis B and/or C virus co-infection had no clinically relevant effect on the exposure to rilpivirine.
Renal Insufficiency: The pharmacokinetics of rilpivirine have not been studied in patients with renal insufficiency. Renal elimination of rilpivirine is negligible. Therefore, the impact of renal impairment on rilpivirine elimination is expected to be minimal. As 99.7% of rilpivirine is bound to plasma, it is unlikely that it will be significantly removed by hemodialysis or peritoneal dialysis (see Renal: Renal Impairment under Precautions and Recommended Dose and Dosage Adjustment: Renal Impairment under Dosage & Administration).
Toxicology: Non-Clinical Toxicology: General Toxicology: Animal toxicology studies have been conducted with rilpivirine in mice, rats, rabbits, dogs and cynomolgus monkeys. The target organs and systems of toxicity were the adrenal cortex and the associated steroid biosynthesis (mouse, rat, dog, cynomolgus monkey), the reproductive organs (female mouse, male and female dog), the liver (mouse, rat, dog), the thyroid and pituitary gland (rat), the kidney (mouse, dog), the hematopoietic system (mouse, rat, dog), and the coagulation system (rat).
Carcinogenesis and Mutagenesis: Rilpivirine was evaluated for carcinogenic potential by oral gavage administration to mice and rats up to 104 weeks. Daily doses of 20, 60 and 160 mg/kg/day were administered to mice, and doses of 40, 200, 500 and 1500 mg/kg/day were administered to rats. An increase in the incidences of hepatocellular adenomas and carcinomas was observed in both mice and rats. An increase in the incidences of follicular cell adenomas and/or carcinomas in the thyroid gland was observed in rats. Administration of rilpivirine did not cause a statistically significant increase in the incidence of any other benign or malignant neoplasm in mice or rats. The observed hepatocellular findings in mice and rats may be rodent-specific, associated with liver enzyme induction. The follicular cell findings may be rat-specific, associated with increased clearance of thyroxine. At the lowest tested doses in the carcinogenicity studies, the systemic exposures (based on AUC) to rilpivirine were 21-fold (mice) and 3-fold (rats), relative to those observed in humans at the recommended dose (25 mg q.d.).
Rilpivirine has tested negative in the in vitro Ames reverse mutation assay, in vitro chromosomal aberration assay in human lymphocyte and in vitro clastogenicity mouse lymphoma assay, tested in the absence and presence of a metabolic activation system. Rilpivirine did not induce chromosomal damage in the in vivo micronucleus test in mice.
Reproductive and Developmental Toxicity: In a study conducted in rats, there were no effects on mating or fertility with rilpivirine up to 400 mg/kg/day, a dose of rilpivirine that showed maternal toxicity. This dose is associated with an exposure that is approximately 40 times higher than the exposure in humans at the recommended dose of 25 mg once daily. Studies in animals have shown no evidence of relevant embryonic or fetal toxicity or an effect on reproductive function at exposures relevant for human administration.
There was no teratogenicity with rilpivirine in rats and rabbits. The exposures at the embryo-fetal No Observed Adverse Effects Levels (NOAELs) in rats and rabbits were respectively 15 and 70 times higher than the exposure in humans at the recommended dose of 25 mg once daily. In a pre- and postnatal development assessment in rats, rilpivirine had no effect on development of off spring during lactation or post weaning when the mothers were dosed up to 400 mg/kg/day.
Impairment of Fertility: No human data on the effect of rilpivirine on fertility are available. In a study conducted in rats, there were no effects on mating or fertility with rilpivirine up to 400 mg/kg/day, a dose of rilpivirine that showed maternal toxicity. This dose is associated with an exposure that is approximately 40 times higher than the exposure in humans at the recommended dose of 25 mg once daily.
Microbiology: Antiviral Activity In Vitro: Rilpivirine exhibited activity against laboratory strains of wild-type HIV-1 in an acutely infected T-cell line with a median EC50 value for HIV-1/IIIB of 0.73 nM (0.27 ng/mL).
Rilpivirine also demonstrated antiviral activity against a broad panel of HIV-1 group M (subtype A, B, C, D, F, G, H) primary isolates with EC50 values ranging from 0.07 to 1.01 nM (0.03 to 0.37 ng/mL) and group O primary isolates with EC50 values ranging from 2.88 to 8.45 nM (1.06 to 3.10 ng/mL).
Rilpivirine showed additive antiviral activity in combination with the N(t)RTIs abacavir, didanosine, emtricitabine, stavudine and tenofovir; the PIs amprenavir, atazanavir, darunavir, indinavir, lopinavir, nelfinavir, ritonavir, saquinavir and tipranavir; the NNRTIs efavirenz, etravirine and nevirapine; the fusion inhibitor enfuvirtide; and the entry inhibitor maraviroc. Rilpivirine shows additive to synergistic antiviral activity in combination with the NRTIs lamivudine and zidovudine, and the integrase inhibitor raltegravir.
Resistance: Resistance In Vitro: Rilpivirine-resistant strains were selected in cell culture starting from wild-type HIV-1 of different origins and subtypes as well as NNRTI resistant HIV-1. The most commonly observed amino acid substitutions that emerged included: L100I, K101E, V108I, E138K, V179F, Y181C, H221Y, F227C and M230I.
Resistance to rilpivirine was determined as a fold change in EC50 value (FC) above the biological cut-off (BCO) of the assay.
Resistance in Treatment-Naïve Adult Subjects: Considering all of the available in vitro and in vivo data, the following amino acid substitutions, when present at baseline, are likely to decrease the antiviral activity of rilpivirine: K101E, K101P, E138A, E138G, E138K, E138R, E138Q, V179L, Y181C, Y181I, Y181V, Y188L, H221Y, F227C, M230I, and M230L.
In the pooled analysis from two Phase III trials, the emergence of resistance among subjects was greater in the EDURANT (rilpivirine) arm as compared to the control (efavirenz) arm at Week 48 (10.6%, 5.3%, respectively) and at Week 96 (14%, 7.6% respectively). Fewer virologic failures due to resistance occurred between Week 48 and Week 96 in each of the treatment arms (3.2% and 2.3% in the rilpivirine and control arms, respectively).
Most common emergent NNRTI substitutions in rilpivirine virologic failures at Week 96 included V90I, K101E/P, E138K/G/Q, V179I/L, Y181I/C, V189I, H221Y, F227C/L and M230L. The E138K substitution emerged most frequently during rilpivirine treatment at Week 48 and Week 96, commonly in combination with the M184I mutation. The most common mutations were the same in the Week 48 and Week 96 analyses.
In the Week 96 pooled analysis of the two Phase III trials, of the 35 subjects with virologic failure on EDURANT and with phenotypic resistance to rilpivirine, 35 (100%) lost susceptibility to lamivudine/emtricitabine. Of the 17 subjects with virologic failure on efavirenz (control) and with phenotypic resistance to efavirenz, 6 (35%) lost susceptibility to lamivudine/emtricitabine. These data were similar to those obtained in the Week 48 pooled analyses.
Cross-resistance: Site-Directed NNRTI Mutant Virus: In a panel of 67 HIV-1 recombinant laboratory strains with one amino acid substitution at RT positions associated with NNRTI resistance, including the most commonly found K103N and Y181C, rilpivirine showed antiviral activity against 64 (96%) of these strains. The single amino acid substitutions associated with a loss of susceptibility to rilpivirine were: K101P, Y181I and Y181V.
The K103N substitution did not show reduced susceptibility to rilpivirine by itself, but the combination of K103N and L100I resulted in a 7-fold reduced susceptibility to rilpivirine.
Recombinant Clinical Isolates: Rilpivirine retained sensitivity (FC ≤ BCO) against 62% of 4786 HIV-1 recombinant clinical isolates resistant to efavirenz and/or nevirapine. Clinical isolates resistant to rilpivirine (FC>BCO) were usually also resistant to etravirine.
Cross-Resistance in Treatment-Naïve Adult Subjects: In the Week 48 pooled analysis of the two Phase III trials, of the 62 subjects with virologic failure on EDURANT for whom phenotypic resistance data was available, 31 (50%) lost susceptibility to rilpivirine and within that subset 28 (90%) were resistant to etravirine, 27 (87%) to efavirenz, and 14 (45%) to nevirapine. Of the 28 subjects with virologic failure on efavirenz (control) for whom phenotypic resistance data was available, 12 (43%) lost susceptibility to efavirenz and within that subset none were resistant to etravirine or to rilpivirine, and 12 (100%) to nevirapine.
In the Week 96 pooled analysis of the two Phase III trials, of the 81 subjects with virologic failure on EDURANT for whom phenotypic resistance data was available, 35 (43%) lost susceptibility to rilpivirine and within that subset 32 (91%) were resistant to etravirine, 30 (86%) to efavirenz, and 16 (45%) to nevirapine. Of the 41 subjects with virologic failure on efavirenz (control) for whom phenotypic resistance data was available, 17 (41%) lost susceptibility to efavirenz and within that subset 1 (6%) were resistant to etravirine, none to rilpivirine, and 15 (88%) to nevirapine.
In the week 96 pooled analyses, among virologic failures in the EDURANT arm with baseline viral load ≤ 100,000 copies/mL and with resistance to rilpivirine, there were fewer patients with phenotypic cross-resistance than among those in the EDURANT arm with baseline viral load > 100,000 copies/mL. 3, 4 and 1 rilpivirine virologic failures with baseline viral load ≤ 100,000 copies/mL and with resistance to rilpivirine (N = 5) had cross-resistance to efavirenz, etravirine and nevirapine, respectively, compared to 27, 28, and 15 rilpivirine virologic failures with baseline viral load > 100,000 copies/mL (N = 30), respectively.