


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Everolimus, a proliferation signal inhibitor, prevents allograft rejection in rodent and non-human primate models of allotransplantation. It exerts its immunosuppressive effect by inhibiting the proliferation, and thus clonal expansion, of antigen-activated T cells which is driven by T cell-specific interleukins, e.g. interleukin-2 and interleukin-15. Everolimus inhibits an intracellular signalling pathway which is triggered upon binding of these T cell growth factors to their respective receptors, and which normally leads to cell proliferation. The blockage of this signal by everolimus leads to an arrest of the cells at the G1 stage of the cell cycle.
At the molecular level, everolimus forms a complex with the cytoplasmic protein FKBP-12. In the presence of everolimus the growth factor-stimulated phosphorylation of the p70 S6 kinase is inhibited. Since p70 S6 kinase phosphorylation is under the control of FRAP (also called m-TOR), this finding suggests that the everolimus-FKBP-12 complex binds to and this interferes with the function of FRAP. FRAP is a key regulatory protein which governs cell metabolism, growth and proliferation; disabling FRAP function thus explains the cell cycle arrest caused by everolimus.
Everolimus, thus, has a different mode of action than ciclosporin. In preclinical models of allotransplantation, the combination of everolimus and ciclosporin was more effective than either compound alone.
The effect of everolimus is not restricted to T cells. It rather inhibits in general growth factor-stimulated proliferation of hematopoietic as well as non-hematopoietic cells, like, for instance, that of vascular smooth muscle cells. Growth factor-stimulated vascular smooth muscle cell proliferation, triggered by injury to endothelial cells and leading to neointima formation, plays a key role in the pathogenesis of chronic rejection. Preclinical studies with everolimus have shown inhibition of neointima formation in a rat aorta allotransplantation model.
Clinical studies: Renal transplantation: Certican in fixed doses of 1.5 mg/day and 3 mg/day, in combination with standard doses of ciclosporin for microemulsion and corticosteroids was investigated in two phase III de novo renal transplant trials (B201 and B251). Mycofenolate mofetil (MMF) 1 g b.i.d was used as comparator. The co-primary composite endpoints were efficacy failure (biopsy-proven acute rejection, graft loss, death or loss to follow-up) at 6 months, and graft loss, death or loss to follow-up at 12 months. Certican was, overall, non-inferior to MMF in these trials. The incidence of biopsy-proven acute rejection at 6 months in the B201 study was 21.6 %, 18.2 %, and 23.5 % for the Certican 1.5 mg/day, Certican 3 mg/day and MMF groups, respectively. In study B251, the incidences were 17.1 %, 20.1 %, and 23.5 % for the Certican 1.5 mg/day, Certican 3 mg/day and MMF groups respectively.
Reduced allograft function with elevated serum creatinine was observed more frequently among subjects using Certican in combination with full dose ciclosporin for microemulsion than in MMF patients. This effect suggests that Certican increases ciclosporin nephrotoxicity. Drug concentration-pharmacodynamic analysis showed that renal function was not impaired with reduced exposure to ciclosporin while conserving efficacy for as long as blood trough everolimus concentration was maintained above 3ng/mL. This concept was subsequently confirmed in two further Phase III studies (A2306 and A2307, including 237 and 256 patients respectively) which evaluated efficacy and safety of Certican 1.5 and 3 mg per day (initial dosing, subsequent dosing based on target trough concentration ≥3 ng/ml) in combination with reduced exposure to ciclosporin. In both studies, renal function was preserved without compromising efficacy. In these studies however there was no non-Certican comparative arm.
A phase III, multicentre, randomised, open-label, controlled trial A2309, has been completed in which 833 de-novo renal transplant recipients were randomised to either one of two Certican regimens, differing by dosage, and combined with reduced-dose ciclosporin or a standard regimen of sodium mycophenolate (MPA) + ciclosporin and treated for 12 months. All patients received induction therapy with basiliximab pre-transplant and on Day 4 post-transplant. Steroids were given as required post-transplant.
Starting dosages in the two Certican groups were 1.5 mg/d and 3 mg, given b.i.d., subsequently modified from Day 5 onwards to maintain target blood trough everolimus levels of 3-8 ng/mL and 6-12 ng/mL respectively. Sodium mycophenolate dosage was 1.44 g/d. Ciclosporin dosages were adapted to maintain target blood trough-level windows as shown in table 1. The actual measured values for blood concentrations of everolimus and ciclosporin (Co and C2) are shown in table 2.
Although the higher dosage Certican regimen was as effective as the lower-dosage regimen, the overall safety was worse and so the upper-dosage regimen is not recommended.
The lower dosage regimen for Certican is that recommended (see Dosage & Administration). (See Table 1 and Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image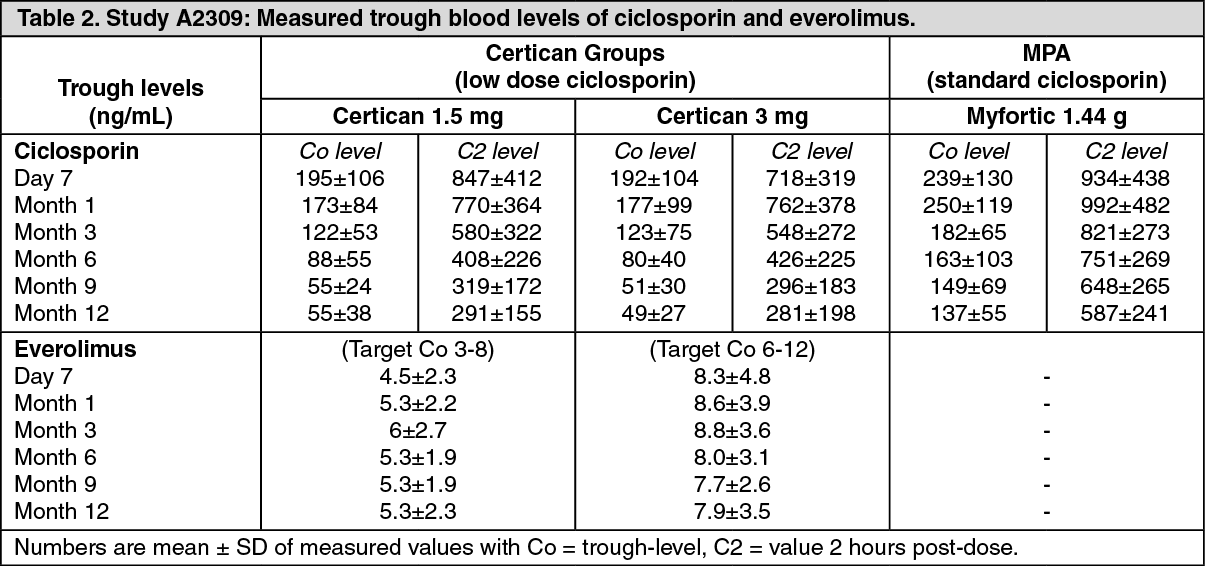 Click on icon to see table/diagram/image
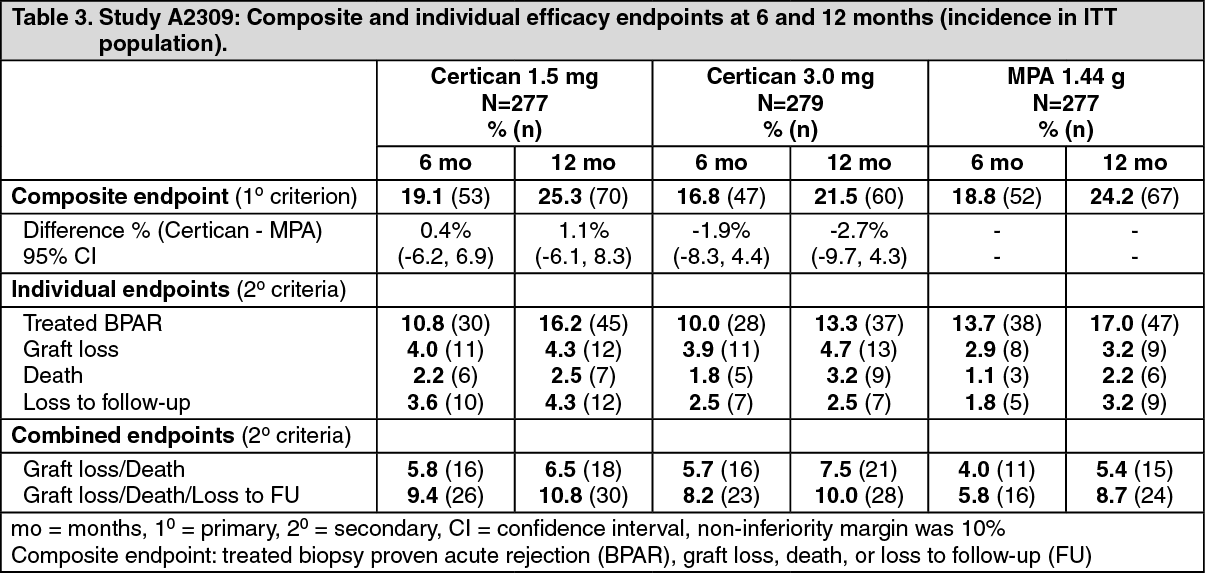
Click on icon to see table/diagram/imageThe primary efficacy endpoint was a composite failure variable (biopsy-proven acute rejection, graft loss, death or loss to follow-up). The outcome is shown in table 3. (See Table 3.)
 Click on icon to see table/diagram/image
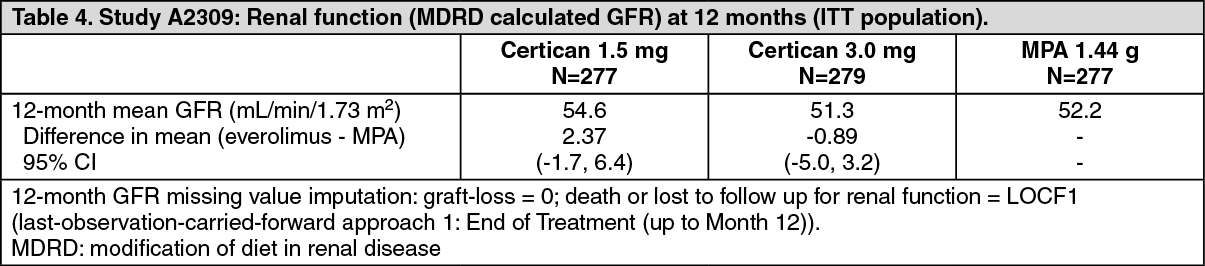
Click on icon to see table/diagram/imageChanges in renal function, as shown by calculated glomerular filtration rate (GFR) using the MDRD formula are shown in table 3.
Proteinuria was assessed at scheduled visits by spot analysis of urinary protein/creatinine (see table 5). A concentration effect was shown relating proteinuria levels to everolimus trough levels particularly at values of Cmin above 8 ng/mL.
Adverse events reported more frequently in the recommended (lower-dosage) Certican regimen than in the MPA control group have been included previously (Table 19). A lower frequency for viral infection was reported for Certican-treated patients resulting principally from lower reporting rates for CMV infection (0.7% versus 5.95%) and BK virus infection (1.5% versus 4.8%). (See Table 4 and Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image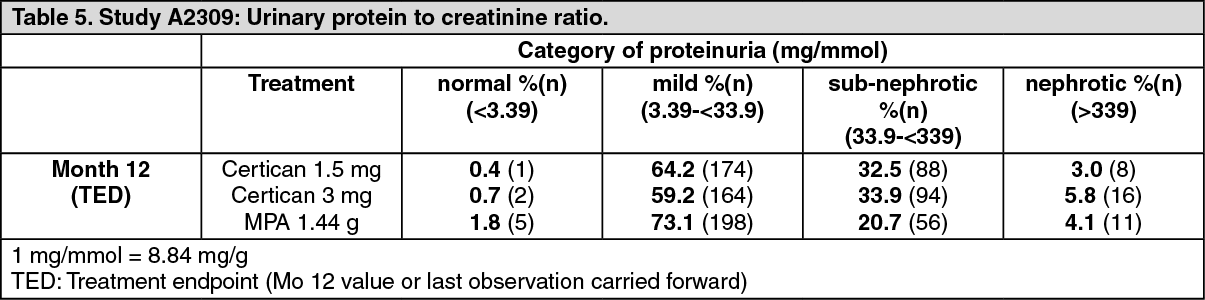 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCardiac transplantation: In the phase III cardiac study (B253), both Certican 1.5 mg/day and 3 mg/day in combination with standard doses of ciclosporin for microemulsion and corticosteroids, was investigated vs. azathioprine (AZA), 1-3 mg/kg/day. The primary endpoint was a composite of incidence of acute rejection ≥ISHLT grade 3A, acute rejection associated with haemodynamic compromise, graft loss, patient death or loss to follow-up at 6, 12 and 24 months. Both doses of Certican were superior to AZA at 6, 12 and 24 months. The incidence of biopsy proven acute rejection ≥ISHLT grade 3A at month 6 was 27.8 % for the 1.5 mg/day group, 19 % for the 3 mg/day group and 41.6% for the AZA group respectively (p = 0.003 for 1.5 mg vs control, < 0.001 for 3 mg vs control).
Based on coronary artery intravascular ultrasound data obtained from a subset of the study population, both Certican doses were statistically significantly more effective than AZA in preventing allograft vasculopathy (defined as an increase in maximum intimal thickness from baseline ≥0.5 mm in at least one matched slice of an automated pullback sequence), an important risk factor for long term graft loss.
Elevated serum creatinine was observed more frequently among subjects using Certican in combination with full dose of ciclosporin for microemulsion than in AZA patients. These results indicated that Certican increases the ciclosporin-induced nephrotoxicity.
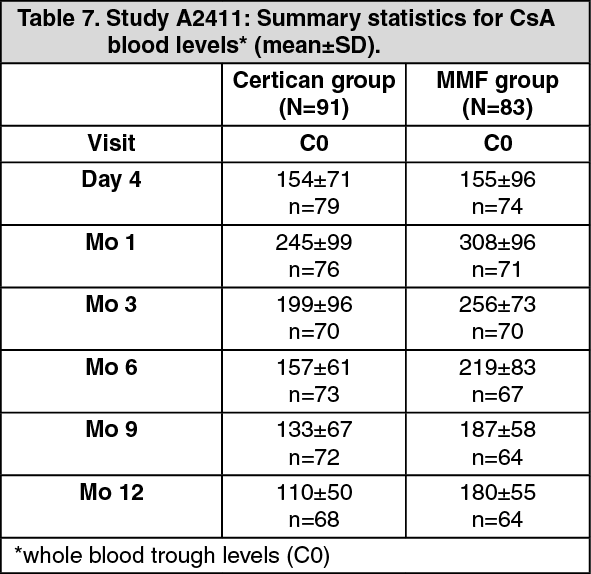
Study A2411 was a randomized, 12 months, open-label study comparing Certican in combination with reduced doses of ciclosporin microemulsion and corticosteroids to mycophenolic mofetil (MMF) and standard doses of ciclosporin microemulsion and corticosteroids in de-novo cardiac transplant patients. Certican was initiated at 1.5 mg/day and the dose was adjusted to maintain target blood everolimus trough levels between 3-8 ng/mL. MMF dosage was initiated at 1,500 mg bid. Ciclosporin microemulsion doses were adjusted to target the following trough levels (ng/mL): (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageActual blood levels measured are shown in table 7. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageChanges in renal functions are shown in table 8. Efficacy outcome is shown in table 9. (See Table 8 and Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image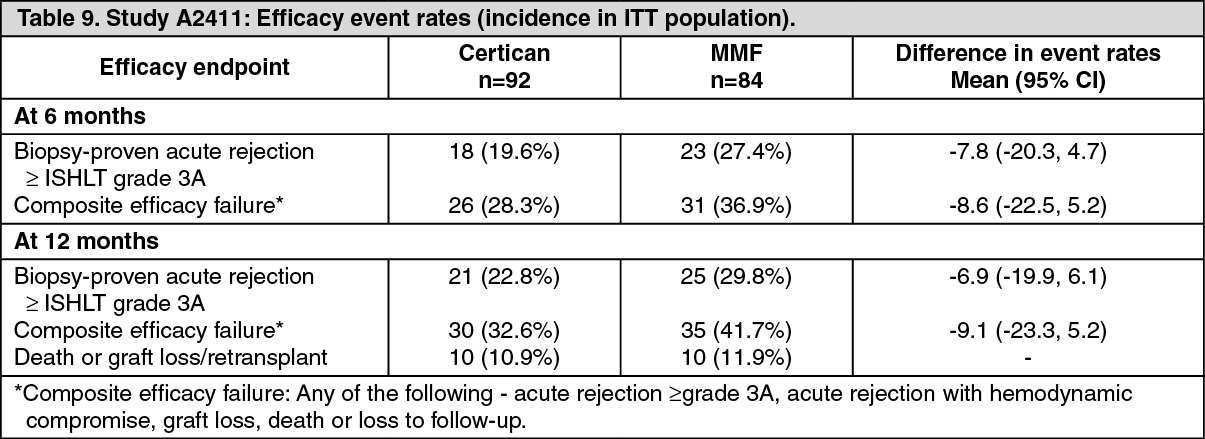 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageStudy A2310 is a phase III, multicenter, randomized, open-label study comparing two Certican/reduced-dose ciclosporin regimens against a standard mycophenolate mofetil (MMF)/ciclosporin regimen over 24 months. The use of induction therapy was center-specific (no-induction or basiliximab or thymoglobulin). All patients received corticosteroids.
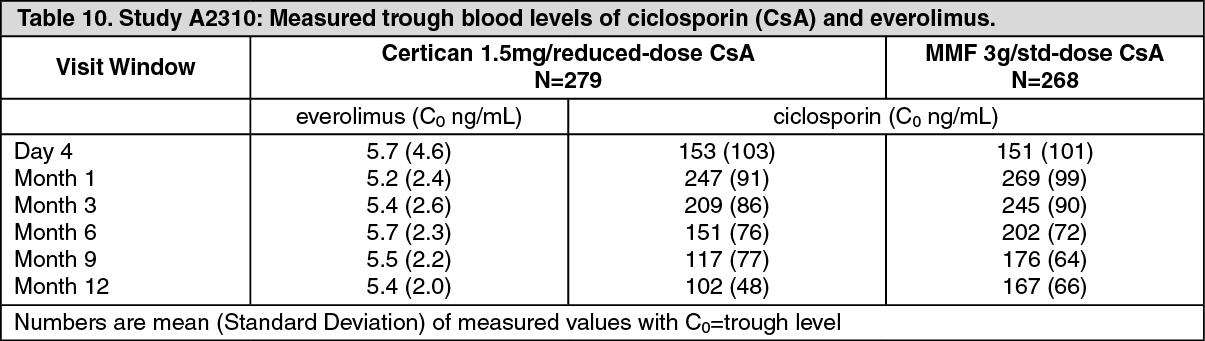
Starting doses in the Certican groups were 1.5 mg/d and 3 mg/d, and were adjusted to target blood trough everolimus levels of 3-8 ng/ml and 6-12 ng/ml respectively. MMF dose was 3 g/d. Ciclosporin dosages targeted the same blood trough levels as in study A2411. Blood concentrations of everolimus and ciclosporin are shown in table 10.
Recruitment to the experimental, upper-dosage Certican treatment arm was prematurely discontinued because of an increased rate of fatalities, due to infection and cardiovascular disorders, occurring within the first 90 days post-randomization. (See Table 10.)
 Click on icon to see table/diagram/image
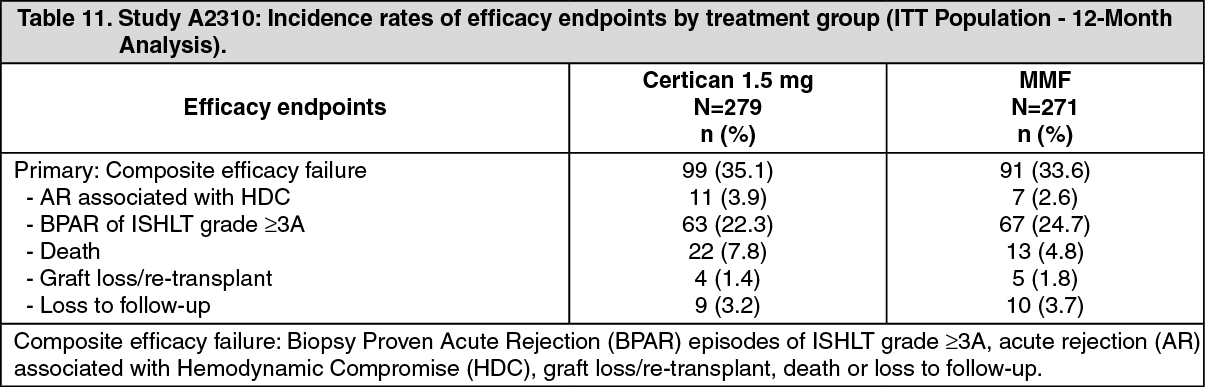
Click on icon to see table/diagram/imageEfficacy outcome at 12 months is shown in Table 11. (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe higher fatality rate in the Certican arm relative to the MMF arm was mainly the result of an increased rate of fatalities from infection in the first three months among Certican patients receiving thymoglobulin induction therapy. The imbalance in fatalities within the thymoglobulin subgroup was particularly evident among patients hospitalized prior to transplantation and with L-ventricular assistance devices (see Precautions).
Renal function over the course of study A2310, assessed by calculated glomerular filtration rate (GFR) using the MDRD formula, was 5.5 mL/min/1.73m2 (97.5% CI -10.9, -0.2) lower for the everolimus 1.5 mg group at Month 12.
This difference was mainly observed in centers where the mean ciclosporin levels were similar throughout the study period in patients receiving Certican and in patients randomized to the control arm. This finding underlines the importance of reducing the ciclosporin levels when combined with everolimus as indicated in the table as follows (see Dosage & Administration): (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditionally, the difference was mainly driven by a difference developed during the first month post-transplantation when patients are still in an unstable hemodynamic situation possibly confounding the analysis of renal function. Thereafter, the decrease in mean GFR from Month 1 to Month 12 was significantly smaller in the everolimus group than in the control group (-6.4 vs -13.7 mL/min, p=0.002).
Proteinuria, expressed as urinary protein: creatinine levels measured in spot urine samples tended to be higher in the Certican-treated patients. Sub-nephrotic values were observed in 22% of the patients receiving Certican compared to MMF patients (8.6%). Nephrotic levels were also reported (0.8%), representing 2 patients in each treatment group (see Precautions).
The adverse reactions for everolimus 1.5 mg group in Study A2310 are consistent with adverse drug reactions presented in table 17. A lower rate of viral infections was reported for Certican-treated patients resulting principally from a lower reporting rate for CMV infection compared to MMF (7.2% vs 19.4%).
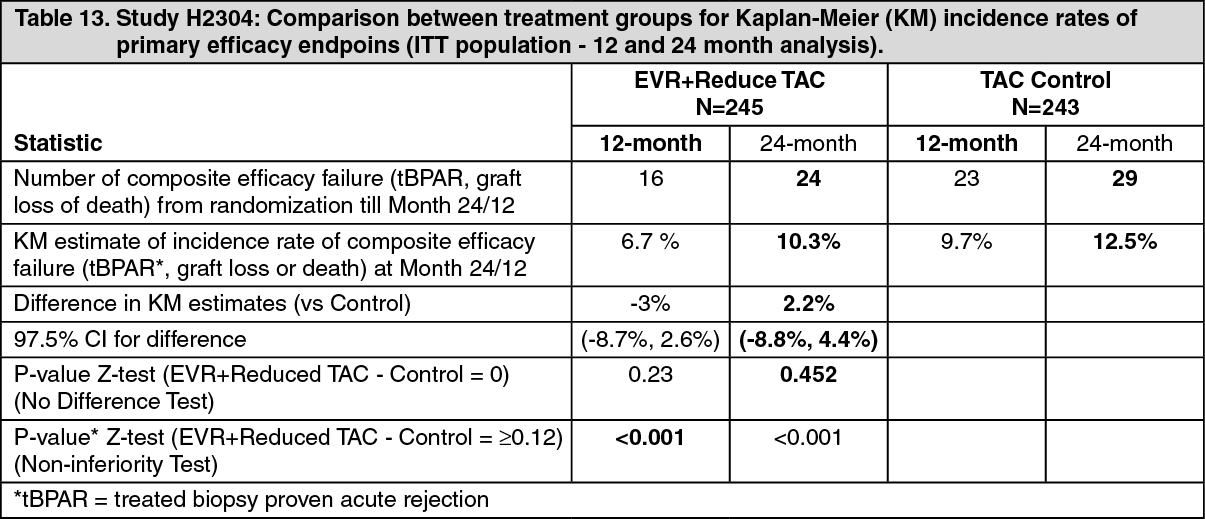
Hepatic transplantation: In the phase III adult hepatic transplant study (H2304), reduced exposure tacrolimus and Certican 1.0 mg twice daily was administered to patients with the initial Certican dose starting approximately 4 weeks after transplantation and was investigated versus standard exposure tacrolimus. Certican was dose adjusted to maintain target blood everolimus trough levels between 3-8 ng/ml for the Certican + reduced tacrolimus arm. Tacrolimus doses were subsequently adjusted to achieve target trough levels between 3-5 ng/ml through 12 months in the Certican + reduced tacrolimus arm.
Overall, in the 12 month analysis, the incidence of the composite endpoint (tBPAR, graft loss or death) was lower in Certican + reduced tacrolimus arm (6.7%) compared to the tacrolimus control arm (9.7%) and consistent results were observed at 24 months (see table 13).
The results of individual components of the composite endpoint are shown in table 14. (See Table 13 and Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image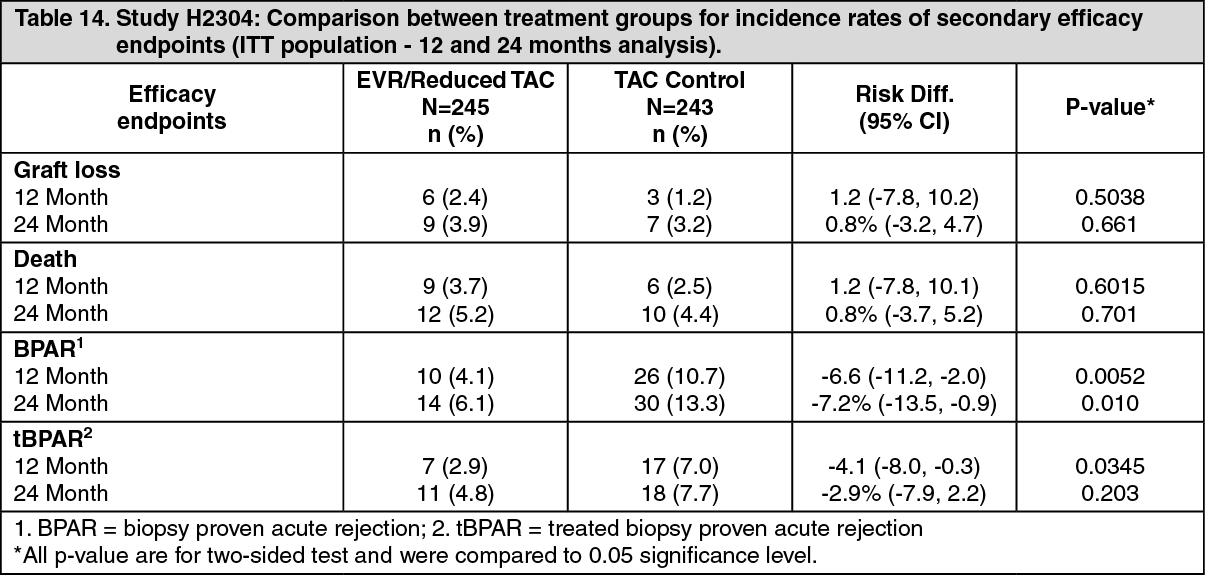 Click on icon to see table/diagram/image
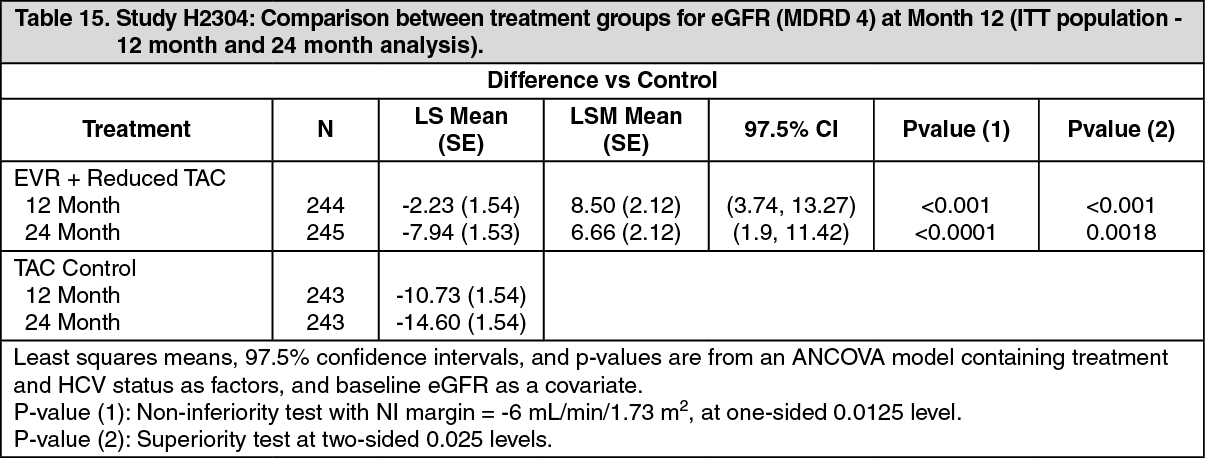
Click on icon to see table/diagram/imageComparison between treatment groups for change in eGFR (MDRD4) [ml/min/1.73 m2] from time of randomization (day 30) to Month 12 and 24 demonstrated superior renal function for Certican + reduced tacrolimus arm (see Table 15).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: After oral dosing, peak everolimus concentrations occur 1 to 2 h postdose. Everolimus blood concentrations are dose proportional over the dose range 0.25 to 15 mg in transplant patients. The relative bioavailability of the dispersible tablet compared with the tablet is 0.90 (90 % CI 0.76-1.07) based on the AUC-ratio. Food effect: Everolimus Cmax and AUC are reduced by 60 % and 16 % when the tablet formulation is given with a high fat meal. To minimize variability, Certican should be taken consistently with or without food.
Distribution: The blood-to-plasma ratio of everolimus is concentration-dependent ranging from 17 % to 73 % over the range of 5 to 5000 ng/ml. Plasma protein binding is approximately 74 % in healthy subjects and patients with moderate hepatic impairment. The distribution volume associated with the terminal phase (Vz/F) in maintenance renal transplant patients is 342 ± 107 l.
Metabolism: Everolimus is a substrate of CYP3A4 and P-glycoprotein. The main metabolic pathways identified in man were mono-hydroxylations and O-dealkylations. Two main metabolites were formed by hydrolysis of the cyclic lactone. Everolimus was the main circulating component in blood. None of the main metabolites are likely to contribute significantly to the immunosuppressive activity of everolimus.
Excretion: After a single dose of radiolabeled everolimus to transplant patients receiving ciclosporin the majority (80 %) of radioactivity was recovered from the faeces, and only a minor amount (5 %) was excreted in urine. Parent drug was not detected in urine and faeces.
Steady-state pharmacokinetics: Pharmacokinetics were comparable for kidney and heart transplant patients receiving everolimus twice daily simultaneously with ciclosporin for microemulsion. Steady-state is reached by day 4 with an accumulation in blood levels of 2 to 3-fold compared with the exposure after the first dose. Tmax occurs at 1 to 2 h postdose. Cmax averages 11.1 ± 4.6 and 20.3 ± 8.0 ng/ml and AUC averages 75 ± 31 and 131 ± 59 ng.h/ml at 0.75 and 1.5 mg bid, respectively. Predose trough blood levels (Cmin) average 4.1 ± 2.1 and 7.1 ± 4.6 ng/ml at 0.75 and 1.5 mg bid, respectively. Everolimus exposure remains stable over time in the first post-transplant year. Cmin is significantly correlated with AUC yielding a correlation coefficient between 0.86 and 0.94. Based on a population pharmacokinetic analysis oral clearance (CL/F) is 8.8 l/h (27 % interpatient variation) and the central distribution volume (Vc/F) is 110 l (36 % interpatient variation). Residual variability in blood concentrations is 31%. The elimination half-life is 28 ± 7 h.
Hepatic impairment: Relative to the AUC of everolimus in subjects with normal hepatic function, the average AUC in 6 patients with mild hepatic impairment (Child-Pugh Class A) was 1.6-fold higher; in two independently studied groups of 8 and 9 patients with moderate hepatic impairment (Child-Pugh Class B) the average AUC was 2.1 fold and 3.3 fold higher respectively; and in 6 patients with severe hepatic impairment (Child-Pugh Class C) the average AUC was 3.6 fold higher. Mean half-lives were 52, 59, and 78 hours in mild, moderate, and severe hepatic impairment. The prolonged half-lives delay the time to reach steady-state everolimus blood levels.
Renal impairment: Post-transplant renal impairment (Clcrea range, 11-107 ml/min) did not affect the pharmacokinetics of everolimus.
Paediatrics: Everolimus CL/F increased in a linear manner with patient age (1 to 16 years), body surface area (0.49-1.92 m2), and weight (11-77 kg). Steady-state CL/F was 10.2 ± 3.0 L/h/m2 and elimination half-life was 30 ± 11 h. Nineteen paediatric de novo renal transplant patients (1 to 16 years) received Certican dispersible tablets at a dose of 0.8 mg/m2 (maximum 1.5 mg) twice-daily with ciclosporin for microemulsion. They achieved an everolimus AUC of 87 ± 27 ng·h/ml which is similar to adults receiving 0.75 mg twice daily. Steady-state trough levels were 4.4 ± 1.7 ng/ml.
Elderly: A limited reduction in everolimus oral CL by 0.33 % per year was estimated in adults (age range studied was 16-70 years). No dose adjustment is considered necessary.
Ethnicity: Based on a population pharmacokinetic analysis, oral clearance (CL/F) is, on average, 20 % higher in Black transplant patients. See Dosage & Administration.
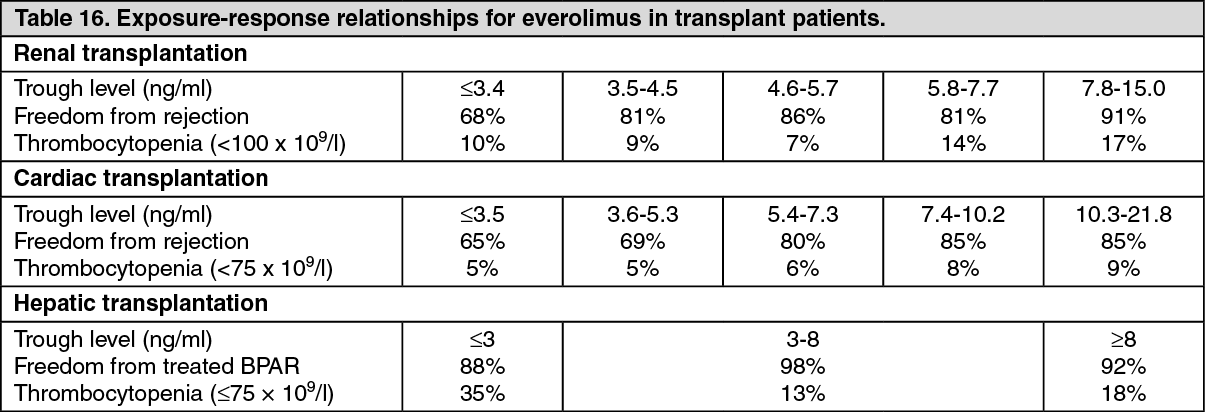
Exposure-response relationships: The average everolimus trough concentration over the first 6 months posttransplant was related to the incidence of biopsy-confirmed acute rejection and of thrombocytopenia in renal and cardiac transplant patients. (see table 16).
In hepatic transplant patients the relationship of the average everolimus trough concentrations and the incidence of biopsy-proven acute rejection is less well defined. No correlation between a higher everolimus exposure and adverse events like thrombocytopenia has been observed (see Table 16).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageToxicology: Preclinical safety data: The preclinical safety profile of everolimus was assessed in mice, rats, minipigs, monkeys and rabbits. The major target organs were male and female reproductive systems (testicular tubular degeneration, reduced sperm content in epididymides and uterine atrophy) in several species, and, only in rats, lungs (increased alveolar macrophages) and eyes (lenticular anterior suture line opacities). Minor kidney changes were seen in the rat (exacerbation of age-related lipofuscin in tubular epithelium) and the mouse (exacerbation of background lesions). There was no indication of kidney toxicity in monkeys or minipigs.
Spontaneously occurring background diseases (chronic myocarditis in the rat, Coxsackie virus infection in plasma and heart in monkeys, coccidial infestation of GI tract in minipigs, skin lesions in mice and monkeys) appeared to be exacerbated by the treatment with everolimus. These findings were generally observed at systemic exposure levels within the range of therapeutic exposure or above, with the exception of findings in rats, which occurred below therapeutic exposure due to a high tissue distribution.
Ciclosporin in combination with everolimus caused higher systemic exposure to everolimus and increased toxicity. There were no new target organs in the rat. Monkeys showed hemorrhage and arteritis in several organs.
In a male fertility study in rats, testicular morphology was affected at 0.5 mg/kg and above, and sperm motility, sperm head count and plasma testosterone levels were diminished at 5 mg/kg which is within the range of therapeutic exposure and caused a decrease in male fertility. There was evidence of reversibility. Female fertility was not affected, but everolimus crossed the placenta and was toxic to the conceptus. In rats, everolimus caused embryo/foetotoxicity, at systemic exposure below the therapeutic one, that was manifested as mortality and reduced foetal weight. The incidence of skeletal variations and malformations at 0.3 and 0.9 mg/kg (e.g. sternal cleft) was increased. In rabbits, embryotoxicity was evident by an increase in late resorptions.
Genotoxicity studies covering relevant genotoxicity end-points showed no evidence of clastogenic or mutagenic activity. Administration of everolimus for up to 2 years did not indicate any oncogenic potential in mice and rats up to the highest doses corresponding respectively to 8.6 and 0.3 times the estimated clinical exposure.