ARCOXIA is a tablet that contains either 30, 60, 90, or 120 mg of etoricoxib as the active ingredient.
Etoricoxib is an oral, selective cyclooxygenase-2 (COX-2) inhibitor within the clinical dose range.
Across clinical pharmacology studies, ARCOXIA produced dose-dependent inhibition of COX-2 without inhibition of COX-1 at doses up to 150 mg daily. Etoricoxib did not inhibit gastric prostaglandin synthesis and had no effect on platelet function.
Cyclooxygenase is responsible for generation of prostaglandins. Two isoforms, COX-1 and COX-2, have been identified. COX-2 is the isoform of the enzyme that has been shown to be induced by pro-inflammatory stimuli and has been postulated to be primarily responsible for the synthesis of prostanoid mediators of pain, inflammation, and fever. COX-2 is also involved in ovulation, implantation and closure of the ductus arteriosus, regulation of renal function, and central nervous system functions (fever induction, pain perception and cognitive function). It may also play a role in ulcer healing. COX-2 has been identified in tissue around gastric ulcers in man but its relevance to ulcer healing has not been established.
ARCOXIA is indicated for: Symptomatic relief of osteoarthritis (OA) and rheumatoid arthritis (RA); Treatment of acute gouty arthritis; Treatment of acute pain, including that related to primary dysmenorrhea; Short-term treatment of moderate pain associated with dental surgery; Symptomatic relief of ankylosing spondylitis.
The decision to prescribe a selective COX-2 inhibitor should be based on an assessment of the individual patient's overall risks (see Precautions).
ARCOXIA is administered orally. ARCOXIA may be taken with or without food. ARCOXIA should be administered for the shortest duration possible and the lowest effective daily dose should be used.
In studies specifically designed to measure the onset of action of etoricoxib, the onset of action occurred as early as 24 minutes after dosing.
Osteoarthritis: The recommended dose is 30 mg or 60 mg once daily.
Rheumatoid Arthritis: The recommended dose is 60 mg once daily. In some patients with insufficient relief from symptoms, an increased dose of 90 mg once daily may increase efficacy. Once the patient is clinically stabilised, down-titration to a 60 mg once daily dose may be appropriate. In the absence of an increase in therapeutic benefit, other therapeutic options should be considered.
Ankylosing Spondylitis: The recommended dose is 60 mg once daily. In some patients with insufficient relief from symptoms, an increased dose of 90 mg once daily may increase efficacy. Once the patient is clinically stabilised, down-titration to a 60 mg once daily dose may be appropriate. In the absence of an increase in therapeutic benefit, other therapeutic options should be considered.
Acute Pain: Acute Gouty Arthritis: The recommended dose is 120 mg once daily.
ARCOXIA 120 mg should be used only for the acute symptomatic period, limited to a maximum of 8 days treatment.
Primary Dysmenorrhea: The recommended dose is 120 mg once daily.
ARCOXIA 120 mg should be used only for the acute symptomatic period, limited to a maximum of 8 days treatment.
Postoperative Dental Surgery Pain: The recommended dose is 90 mg once daily.
ARCOXIA should be used only for the acute symptomatic period, limited to a maximum of 3 days treatment. Some patients may require additional postoperative analgesia.
Doses greater than those recommended for each indication have either not demonstrated additional efficacy or have not been studied. Therefore: The dose for OA should not exceed 60 mg daily. The dose for RA should not exceed 90 mg daily. The dose for ankylosing spondylitis should not exceed 90 mg daily. The dose for acute gout should not exceed 120 mg daily. The dose for primary dysmenorrhea should not exceed 120 mg daily. The dose for postoperative dental surgery pain should not exceed 90 mg daily.
As the cardiovascular risks of selective COX-2 inhibitors may increase with dose and duration of exposure, the shortest duration possible and the lowest effective daily dose should be used. The patient's need for symptomatic relief and response to therapy should be re-evaluated periodically. (See Precautions.)
Elderly, Gender, Race: No dosage adjustment in ARCOXIA is necessary for the elderly or based on gender or race.
Hepatic Insufficiency: In patients with mild hepatic insufficiency (Child-Pugh score 5-6), a dose of 60 mg once daily should not be exceeded. In patients with moderate hepatic insufficiency (Child-Pugh score 7-9), the dose should be reduced; a dose of 60 mg every other day should not be exceeded, administration of 30 mg once daily can also be considered. There is no clinical experience in patients with severe hepatic dysfunction (Child-Pugh score ≥10); therefore, its use is contraindicated in these patients. (See Contraindications and Precautions.)
Renal Insufficiency: The use of etoricoxib in patients with advanced renal disease (creatinine clearance <30 mL/min) is contraindicated (see Contraindications). No dosage adjustment is necessary for patients with lesser degrees of renal insufficiency (creatinine clearance ≥30 mL/min). (See Precautions.)
In clinical studies, administration of single doses of etoricoxib up to 500 mg and multiple doses up to 150 mg/day for 21 days did not result in significant toxicity. There have been reports of acute overdosage with etoricoxib, although adverse experiences were not reported in the majority of cases. The most frequently observed adverse experiences were consistent with the safety profile for etoricoxib (e.g. gastrointestinal events, cardiorenal events).
In the event of overdose, it is reasonable to employ the usual supportive measures, e.g., remove unabsorbed material from the GI tract, employ clinical monitoring, and institute supportive therapy, if required.
Etoricoxib is not dialyzable by hemodialysis; it is not known whether etoricoxib is dialyzable by peritoneal dialysis.
Hypersensitivity to the active substance or to any of the excipients.
Active peptic ulceration or active gastrointestinal (GI) bleeding.
Patients who, after taking acetylsalicylic or NSAIDs including COX-2 (cyclooxygenase-2) inhibitors, experience bronchospasm, acute rhinitis, nasal polyps, angioneurotic oedema, urticaria, or allergic-type reactions.
Pregnancy and lactation (see Pregnancy and Nursing Mothers under Use in Pregnancy & Lactation).
Severe hepatic dysfunction (serum albumin <25 g/l or Child-Pugh score ≥10).
Estimated renal creatinine clearance <30 mL/min.
Children and adolescents under 16 years of age.
Inflammatory bowel disease.
Congestive heart failure (NYHA II-IV).
Patients with hypertension whose blood pressure is persistently elevated above 140/90 mmHg and has not been adequately controlled.
Established ischaemic heart disease, peripheral arterial disease, and/or cerebrovascular disease.
Treatment of peri-operative pain in the setting of coronary artery bypass graft surgery.
Gastrointestinal effects: NSAIDs cause an increased risk of serious gastrointestinal adverse events including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients are at greater risk for serious gastrointestinal events.
There is a further increase in the risk of gastrointestinal adverse effects (gastrointestinal ulceration or other gastrointestinal complications) when etoricoxib is taken concomitantly with acetylsalicylic acid (even at low doses). A significant difference in GI safety between selective COX-2 inhibitors + acetylsalicylic acid vs. NSAIDs + acetylsalicylic acid has not been demonstrated in long-term clinical trials.
Cardiovascular effects: NSAIDs may cause an increased risk of serious cardiovascular thrombotic events, myocardial infarction, and stroke, which can be fatal. This risk may increase with duration of use. Patients with cardiovascular disease or risk factors for cardiovascular disease may be at greater risk. As the cardiovascular risks of etoricoxib may increase with dose and duration of exposure, the shortest duration possible and the lowest effective daily dose should be used. The patient's need for symptomatic relief and response to therapy should be re-evaluated periodically, especially in patients with osteoarthritis (see Dosage & Administration, Contraindications, and Side Effects).
Patients with significant risk factors for cardiovascular events (e.g. hypertension, hyperlipidaemia, diabetes mellitus, smoking) should only be treated with etoricoxib after careful consideration.
COX-2 selective inhibitors are not a substitute for acetylsalicylic acid for prophylaxis of cardiovascular thromboembolic diseases because of their lack of antiplatelet effect. Therefore, antiplatelet therapies should not be discontinued (see Interactions).
Renal effects: Long-term administration of NSAIDs has resulted in renal papillary necrosis and other renal injury. Renal toxicity has also been seen in patients in whom renal prostaglandins have a compensatory role in the maintenance of renal perfusion. In these patients, administration of a NSAID may cause a dose-dependent reduction in prostaglandin formation and, secondarily, in renal blood flow, which may precipitate overt renal decompensation. Patients at greatest risk of this reaction are those with impaired renal function, heart failure, liver dysfunction, those taking diuretics and ACE inhibitors, and the elderly. Discontinuation of NSAID therapy is usually followed by recovery to the pretreatment state. Monitoring of renal function in such patients should be considered.
Advanced renal disease: No information is available from controlled clinical studies regarding the use of ARCOXIA in patients with advanced renal disease. Therefore, treatment with ARCOXIA is contraindicated in patients with advanced renal disease (estimated renal creatinine clearance <30 mL/min) (see Contraindications and Dosage & Administration).
Fluid retention, oedema and hypertension: As with other medicinal products known to inhibit prostaglandin synthesis, fluid retention, oedema and hypertension have been observed in patients taking etoricoxib. All nonsteroidal anti-inflammatory drugs (NSAIDs), including etoricoxib, can be associated with new onset or recurrent congestive heart failure. Caution should be exercised in patients with a history of cardiac failure, left ventricular dysfunction, or hypertension and in patients with pre-existing oedema from any other reason. If there is clinical evidence of deterioration in the condition of these patients, appropriate measures including discontinuation of etoricoxib should be taken.
Etoricoxib may be associated with more frequent and severe hypertension than some other NSAIDs and selective COX-2 inhibitors, particularly at high doses. Therefore, hypertension should be controlled before treatment with etoricoxib (see Contraindications) and special attention should be paid to blood pressure monitoring during treatment with etoricoxib. Blood pressure should be monitored within two weeks after initiation of treatment and periodically thereafter. If blood pressure rises significantly, alternative treatment should be considered.
Hepatic effects: Elevations of alanine aminotransferase (ALT) and/or aspartate aminotransferase (AST) (approximately three or more times the upper limit of normal) have been reported in approximately 1% of patients in clinical trials treated for up to one year with etoricoxib 30, 60 and 90 mg daily.
Warning: In rare cases, etoricoxib has been associated with serious liver injury. Any patients with symptoms and/or signs suggesting liver dysfunction, or in whom an abnormal liver function test has occurred, should be monitored. If signs of hepatic insufficiency occur, or if persistently abnormal liver function tests (three times the upper limit of normal) are detected, etoricoxib should be discontinued.
General: If during treatment, patients deteriorate in any of the organ system functions described previously, appropriate measures should be taken and discontinuation of etoricoxib therapy should be considered. Medically appropriate supervision should be maintained when using etoricoxib in the elderly and in patients with renal, hepatic, or cardiac dysfunction.
Caution should be used when initiating treatment with etoricoxib in patients with dehydration. It is advisable to rehydrate patients prior to starting therapy with etoricoxib.
Serious skin reactions, some of them fatal, including exfoliative dermatitis, Stevens-Johnson syndrome, and toxic epidermal necrolysis, have been reported very rarely in association with the use of NSAIDs and some selective COX-2 inhibitors during post-marketing surveillance (see Side Effects). Patients appear to be at highest risk for these reactions early in the course of therapy with the onset of the reaction occurring in the majority of cases within the first month of treatment. Serious hypersensitivity reactions (such as anaphylaxis and angioedema) have been reported in patients receiving etoricoxib (see Side Effects). Some selective COX-2 inhibitors have been associated with an increased risk of skin reactions in patients with a history of any drug allergy. Etoricoxib should be discontinued at the first appearance of skin rash, mucosal lesions, or any other sign of hypersensitivity.
Etoricoxib may mask fever and other signs of inflammation.
Caution should be exercised when co-administering etoricoxib with warfarin or other oral anticoagulants (see Interactions).
The use of etoricoxib, as with any medicinal product known to inhibit cyclooxygenase/prostaglandin synthesis, is not recommended in women attempting to conceive (see Fertility under Use in Pregnancy & Lactation).
ARCOXIA tablets contain lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and use machines: Patients who experience dizziness, vertigo or somnolence while taking etoricoxib should refrain from driving or operating machinery.
Use in Children: Etoricoxib is contraindicated in children and adolescents under 16 years of age (see Contraindications). Safety and effectiveness of etoricoxib in pediatric patients have not been established.
The pharmacokinetics of etoricoxib in pediatric patients (<12 years of age) have not been studied. In a pharmacokinetic study (N=16) conducted in adolescents (aged 12 to 17), the pharmacokinetics in adolescents weighing 40 to 60 kg given etoricoxib 60 mg once daily and in adolescents >60 kg given etoricoxib 90 mg once daily were similar to the pharmacokinetics in adults given etoricoxib 90 mg once daily.
Use in the Elderly: Pharmacokinetics in the elderly (65 years of age and older) are similar to those in the young. In clinical studies, a higher incidence of adverse experiences was seen in older patients compared to younger patients; the relative differences between etoricoxib and control groups were similar in the elderly and the young. Greater sensitivity of some older individuals cannot be ruled out.
Pregnancy: No clinical data on exposed pregnancies are available for etoricoxib. Studies in animals have shown reproductive toxicity. The potential for human risk in pregnancy is unknown. Etoricoxib, as with other medicinal products inhibiting prostaglandin synthesis, may cause uterine inertia and premature closure of the ductus arteriosus during the last trimester. Etoricoxib is contraindicated in pregnancy (see Contraindications). If a woman becomes pregnant during treatment, etoricoxib must be discontinued.
Published studies and post-marketing reports describe maternal nonsteroidal anti-inflammatory drug (NSAID) use at approximately 20 weeks gestation or later in pregnancy associated with fetal renal dysfunction leading to oligohydramnios, and in some cases, neonatal renal impairment or failure. NSAIDs were shown to cause significant reduction in fetal urine production prior to reduction of amniotic fluid volume. There have also been a limited number of case reports of maternal NSAID use and neonatal renal dysfunction and renal impairment without oligohydramnios, some of which were irreversible, even after treatment discontinuation.
These adverse outcomes are seen, on average, after days to weeks of treatment, although oligohydramnios has been infrequently reported as soon as 48 hours after NSAID initiation.
Complications of prolonged oligohydramnios may for example, include limb contractures and delayed lung maturation. In some post-marketing cases of impaired neonatal renal function, invasive procedures such as exchange transfusion or dialysis were required.
Fertility: The use of etoricoxib, as with any drug substance known to inhibit COX-2, is not recommended in women attempting to conceive.
Nursing Mothers: It is not known whether etoricoxib is excreted in human milk. Etoricoxib is excreted in the milk of lactating rats. Women who use etoricoxib must not breastfeed (see Contraindications).
Summary of the safety profile: In clinical trials, etoricoxib was evaluated for safety in 9295 individuals, including 6757 patients with OA, RA, chronic low back pain or ankylosing spondylitis (approximately 600 patients with OA or RA were treated for one year or longer).
In clinical studies, the undesirable effects profile was similar in patients with OA or RA treated with etoricoxib for one year or longer.
In a clinical study for acute gouty arthritis, patients were treated with etoricoxib 120 mg once daily for eight days. The adverse experience profile in this study was generally similar to that reported in the combined OA, RA, and chronic low back pain studies.
In a cardiovascular safety outcomes program of pooled data from three active comparator controlled trials, 17,412 patients with OA or RA were treated with etoricoxib (60 mg or 90 mg) for a mean duration of approximately 18 months.
In clinical studies for acute postoperative dental pain following surgery including 614 patients treated with etoricoxib (90 mg or 120 mg), the adverse experience profile in these studies was generally similar to that reported in the combined OA, RA, and chronic low back pain studies.
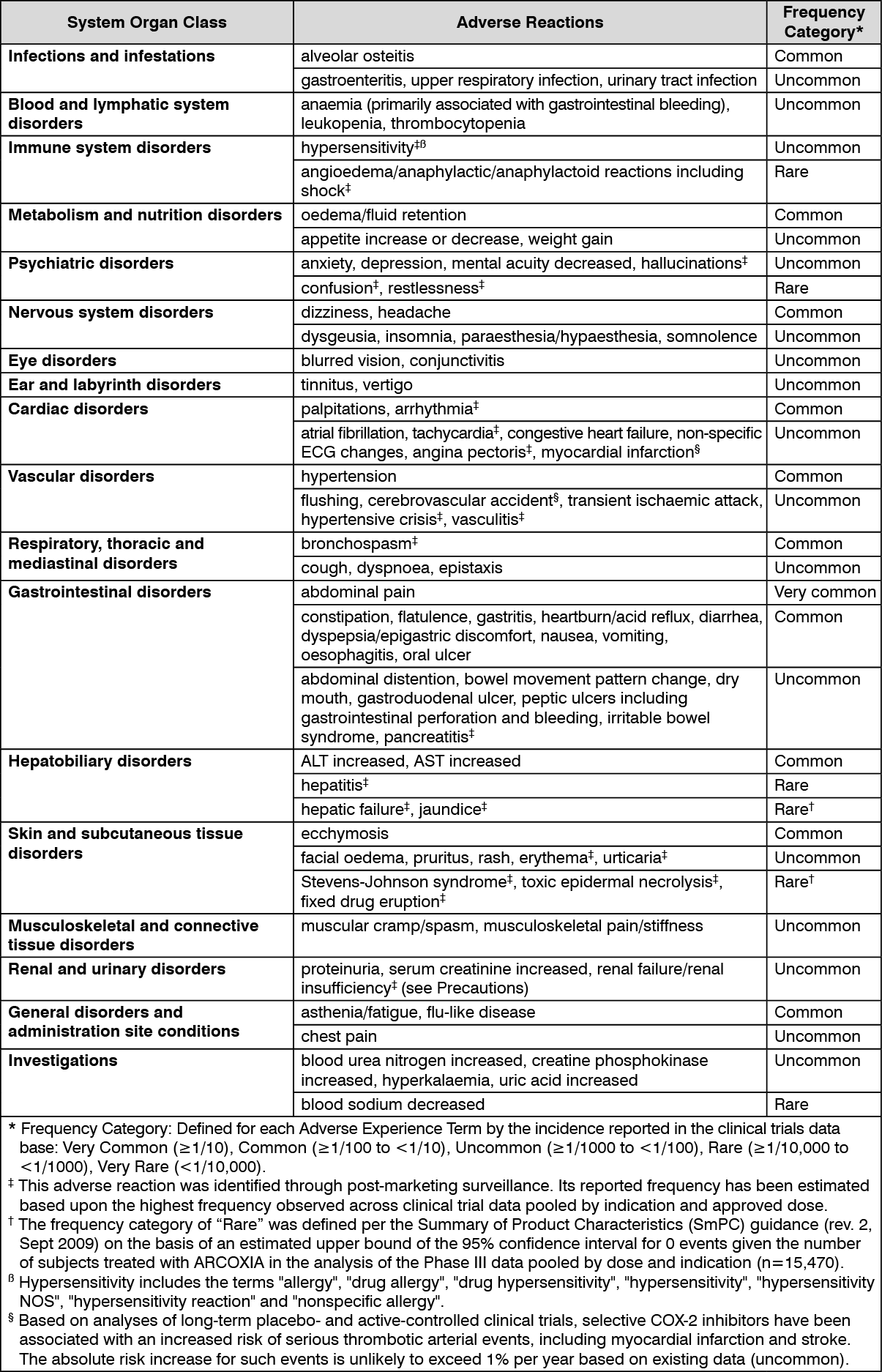
Tabulated list of adverse reactions: The following undesirable effects were reported at an incidence greater than placebo in clinical trials in patients with OA, RA, chronic low back pain or ankylosing spondylitis treated with etoricoxib 30 mg, 60 mg or 90 mg up to the recommended dose for up to 12 weeks; in the MEDAL Program studies for up to 3½ years; in short-term acute pain studies for up to 7 days; or in post-marketing experience: See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The following serious undesirable effects have been reported in association with the use of NSAIDs and cannot be ruled out for etoricoxib: nephrotoxicity including interstitial nephritis and nephrotic syndrome.
Pharmacodynamic interactions: Oral anticoagulants: In subjects stabilised on chronic warfarin therapy, the administration of etoricoxib 120 mg daily was associated with an approximate 13% increase in prothrombin time International Normalised Ratio (INR). Therefore, patients receiving oral anticoagulants should be closely monitored for their prothrombin time INR, particularly in the first few days when therapy with etoricoxib is initiated or the dose of etoricoxib is changed (see Precautions).
Diuretics, ACE inhibitors and angiotensin II antagonists: NSAIDs may reduce the effect of diuretics and other antihypertensive drugs. In some patients with compromised renal function (e.g. dehydrated patients or elderly patients with compromised renal function), the co-administration of an ACE inhibitor or angiotensin II antagonist and agents that inhibit cyclooxygenase may result in further deterioration of renal function, including possible acute renal failure, which is usually reversible. These interactions should be considered in patients taking etoricoxib concomitantly with ACE inhibitors or angiotensin II antagonists. Therefore, the combination should be administered with caution, especially in the elderly. Patients should be adequately hydrated and consideration should be given to monitoring of renal function after initiation of concomitant therapy, and periodically thereafter.
Acetylsalicylic acid: In a study in healthy subjects, at steady state, etoricoxib 120 mg once daily had no effect on the antiplatelet activity of acetylsalicylic acid (81 mg once daily). Etoricoxib can be used concomitantly with acetylsalicylic acid at doses used for cardiovascular prophylaxis (low-dose acetylsalicylic acid). However, concomitant administration of low-dose acetylsalicylic acid with etoricoxib may result in an increased rate of GI ulceration or other complications compared to use of etoricoxib alone. Concomitant administration of etoricoxib with doses of acetylsalicylic acid above those for cardiovascular prophylaxis or with other NSAIDs is not recommended (see Precautions).
Cyclosporine and tacrolimus: Although this interaction has not been studied with etoricoxib, co-administration of cyclosporine or tacrolimus with any NSAID may increase the nephrotoxic effect of cyclosporine or tacrolimus. Renal function should be monitored when etoricoxib and either of these drugs is used in combination.
Pharmacokinetic interactions: Effect of etoricoxib on the pharmacokinetics of other drugs: Lithium: NSAIDs decrease lithium renal excretion and therefore increase lithium plasma levels. If necessary, monitor blood lithium closely and adjust the lithium dosage while the combination is being taken and when the NSAID is withdrawn.
Methotrexate: Two studies investigated the effects of etoricoxib 60, 90 or 120 mg administered once daily for seven days in patients receiving once-weekly methotrexate doses of 7.5 to 20 mg for rheumatoid arthritis. Etoricoxib at 60 and 90 mg had no effect on methotrexate plasma concentrations or renal clearance. In one study, etoricoxib 120 mg had no effect, but in the other study, etoricoxib 120 mg increased methotrexate plasma concentrations by 28% and reduced renal clearance of methotrexate by 13%. Adequate monitoring for methotrexate-related toxicity is recommended when etoricoxib and methotrexate are administered concomitantly.
Oral contraceptives: Etoricoxib 60 mg given concomitantly with an oral contraceptive containing 35 micrograms ethinyl estradiol (EE) and 0.5 to 1 mg norethindrone for 21 days increased the steady-state AUC0-24hr of EE by 37%. Etoricoxib 120 mg given with the same oral contraceptive concomitantly or separated by 12 hours, increased the steady-state AUC0-24hr of EE by 50 to 60%. This increase in EE concentration should be considered when selecting an oral contraceptive for use with etoricoxib. An increase in EE exposure can increase the incidence of adverse events associated with oral contraceptives (e.g., venous thromboembolic events in women at risk).
Hormone replacement therapy (HRT): Administration of etoricoxib 120 mg with hormone replacement therapy consisting of conjugated estrogens (0.625 mg PREMARIN) for 28 days increased the mean steady-state AUC0-24hr of unconjugated estrone (41%), equilin (76%), and 17β-estradiol (22%). The effect of the recommended chronic doses of etoricoxib (30, 60, and 90 mg) has not been studied. The effects of etoricoxib 120 mg on the exposure (AUC0-24hr) to these estrogenic components of PREMARIN were less than half of those observed when PREMARIN was administered alone and the dose was increased from 0.625 to 1.25 mg. The clinical significance of these increases is unknown, and higher doses of PREMARIN were not studied in combination with etoricoxib. These increases in estrogenic concentration should be taken into consideration when selecting post-menopausal hormone therapy for use with etoricoxib because the increase in estrogen exposure might increase the risk of adverse events associated with HRT.
Prednisone/prednisolone: In drug interaction studies, etoricoxib did not have clinically important effects on the pharmacokinetics of prednisone/prednisolone.
Digoxin: Etoricoxib 120 mg administered once daily for 10 days to healthy volunteers did not alter the steady-state plasma AUC0-24hr or renal elimination of digoxin. There was an increase in digoxin Cmax (approximately 33%). This increase is not generally important for most patients. However, patients at high risk of digoxin toxicity should be monitored for this when etoricoxib and digoxin are administered concomitantly.
Effect of etoricoxib on drugs metabolised by sulfotransferases: Etoricoxib is an inhibitor of human sulfotransferase activity, particularly SULT1E1, and has been shown to increase the serum concentrations of ethinyl estradiol. While knowledge about effects of multiple sulfotransferases is presently limited and the clinical consequences for many drugs are still being examined, it may be prudent to exercise care when administering etoricoxib concurrently with other drugs primarily metabolised by human sulfotransferases (e.g., oral salbutamol and minoxidil).
Effect of etoricoxib on drugs metabolised by CYP isoenzymes: Based on in vitro studies, etoricoxib is not expected to inhibit cytochromes P450 (CYP) 1A2, 2C9, 2C19, 2D6, 2E1 or 3A4. In a study in healthy subjects, daily administration of etoricoxib 120 mg did not alter hepatic CYP3A4 activity as assessed by the erythromycin breath test.
Effects of other drugs on the pharmacokinetics of etoricoxib: The main pathway of etoricoxib metabolism is dependent on CYP enzymes. CYP3A4 appears to contribute to the metabolism of etoricoxib in vivo. In vitro studies indicate that CYP2D6, CYP2C9, CYP1A2 and CYP2C19 also can catalyse the main metabolic pathway, but their quantitative roles have not been studied in vivo.
Ketoconazole: Ketoconazole, a potent inhibitor of CYP3A4, dosed at 400 mg once a day for 11 days to healthy volunteers, did not have any clinically important effect on the single-dose pharmacokinetics of 60 mg etoricoxib (43% increase in AUC).
Voriconazole and miconazole: Co-administration of either oral voriconazole or topical miconazole oral gel, strong CYP3A4 inhibitors, with etoricoxib caused a slight increase in exposure to etoricoxib, but is not considered to be clinically meaningful based on published data.
Rifampin: Co-administration of etoricoxib with rifampin, a potent inducer of CYP enzymes, produced a 65% decrease in etoricoxib plasma concentrations. This interaction may result in recurrence of symptoms when etoricoxib is co-administered with rifampin. While this information may suggest an increase in dose, doses of etoricoxib greater than those listed for each indication have not been studied in combination with rifampin and are therefore not recommended (see Dosage & Administration).
Antacids: Antacids do not affect the pharmacokinetics of etoricoxib to a clinically relevant extent.
Do not throw away any medicines via wastewater or household waste. Ask the pharmacist how to throw away medicines no longer used. These measures will help protect the environment.
Store in the original package in order to protect from moisture.
M01AH05 - etoricoxib ; Belongs to the class of non-steroidal antiinflammatory and antirheumatic products, coxibs.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
