Adult: For the relief of symptoms of dry or irritating coughs: 15-30 mg 3-4 times daily. Dosage and treatment recommendations may vary among individual products and between countries (refer to detailed product guidelines). Elderly: Dose reduction may be needed.
Oral Acute diarrhoea
Adult: For symptomatic relief: 15-60 mg 3-4 times daily. Elderly: Dose reduction may be needed. Child: ≥12 years 30-60 mg or 0.5-1 mg/kg 6 hourly up to Max 240 mg daily, if needed. Max treatment duration: 3 days. Dosage is individualised based on the severity of pain, patient response, opioid tolerance, and prior analgesic experience. Use the lowest effective dose for the shortest possible duration. Dosage and treatment recommendations may vary among individual products and between countries (refer to detailed product guidelines).
Oral Mild to moderate pain
Adult: For the management of cases in which alternative treatments are inadequate: 15-60 mg 4-6 hourly. Max: 240 mg daily. Max treatment duration: 3 days. Dosage is individualised based on the severity of pain, patient response, opioid tolerance, and prior analgesic experience. Use the lowest effective dose for the shortest possible duration. Dosage and treatment recommendations may vary among individual products and between countries (refer to detailed product guidelines). Elderly: Dose reduction may be needed. Child: ≥12 years For the management of cases in which alternative treatments are inadequate: 30-60 mg or 0.5-1 mg/kg 6 hourly up to Max 240 mg daily, if needed. Max treatment duration: 3 days. Dosage is individualised based on the severity of pain, patient response, opioid tolerance, and prior analgesic experience. Use the lowest effective dose for the shortest possible duration. Dosage and treatment recommendations may vary among individual products and between countries (refer to detailed product guidelines).
Nhóm bệnh nhân đặc biệt
Cachectic or debilitated patients: Dose reduction may be needed.
Pharmacogenomics:
Codeine, an opioid analgesic prodrug, is metabolised via O-demethylation by the CYP2D6 isoenzyme to its active metabolite, morphine. Polymorphisms in the CYP2D6 gene may result in higher morphine levels which may lead to toxic systemic concentrations of morphine even in low doses or a decrease in morphine levels that eventually cause an attenuated analgesic effect. Genetic testing should be considered for children and adults before initiation of codeine therapy to identify those with a predisposition to adverse effects from codeine use.
Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline as of December 2020:
Phenotype
Implications
Recommendations
CYP2D6 ultrarapid metaboliser
Increased morphine formation, thereby increasing the risk of toxicity.
Avoid codeine administration. Consider the administration of non-tramadol opioids if opioid use is desired.
CYP2D6 intermediate metaboliser
Reduced morphine formation.
No dose adjustment needed. If there is no response and opioid use is desired, consider the administration of non-tramadol opioids.
CYP2D6 poor metaboliser
Greatly reduced morphine formation, resulting in decreased analgesia.
Avoid codeine administration. Consider the administration of non-tramadol opioids if opioid use is desired.
Suy thận
Dose reduction may be needed.
Suy gan
Mild to moderate: Dose reduction may be needed. Severe: Contraindicated.
Cách dùng
May be taken with or without food.
Chống chỉ định
Significant respiratory depression, acute or severe bronchial asthma (in unmonitored setting or lack of resuscitative equipment), moderate to severe sleep-disordered breathing, impaired consciousness or comatose patients, head injury, conditions in which intracranial pressure is elevated, gastrointestinal obstruction including risk of or known paralytic ileus, conditions where abdominal distension develops, diarrhoea caused by poisoning or antibiotic-associated colitis (e.g. pseudomembranous colitis). Severe hepatic impairment. Children <12 years old; <18 years old undergoing tonsillectomy and/or adenoidectomy for obstructive sleep apnoea. CYP2D6 ultrarapid and poor metabolisers. Lactation. Concomitant or within 14 days after MAOI therapy.
Thận trọng
Patient with hypersensitivity to other phenanthrene-derivative opioid agonists (e.g. hydrocodone, hydromorphone, levorphanol, oxycodone, oxymorphone), current or history of asthma, respiratory disease (e.g. significant COPD or cor pulmonale, decreased respiratory reserve, hypoxia, hypercarbia, or pre-existing respiratory depression), intestinal motility disorders, biliary tract dysfunction (including acute pancreatitis), inflammatory or obstructive bowel disorders, adrenocortical insufficiency (including Addison's disease), thyroid dysfunction (e.g. hypothyroidism), shock, hypotension, hypovolaemia, CV disease (including acute or post-MI, unstable angina), prostatic hypertrophy and/or urethral stricture, delirium tremens, toxic psychosis, history of seizure disorders, current or history of substance abuse and mental health conditions (e.g. anxiety disorders, depression, PTSD), sleep-related disorders including sleep apnoea, myasthenia gravis. Patient in the perioperative setting. Not recommended for long-term use. Not recommended for use in children in whom respiratory function may be compromised (e.g. neuromuscular disorders, multiple trauma or extensive surgical procedures, upper respiratory or lung infections, severe cardiac or respiratory conditions). Avoid abrupt withdrawal. Concomitant use of sedative medicines including benzodiazepines or other CNS depressants. CYP2D6 intermediate metabolisers. Morbidly obese, cachectic, or debilitated patients. Renal and mild to moderate hepatic impairment. Children and elderly. Pregnancy.
Tác dụng không mong muốn
Significant: CNS depression, constipation, obstructive bowel disease (chronic use), opioid-induced hyperalgesia, severe hypotension including syncope and orthostatic hypotension, secondary hypogonadism (long-term use) which may lead to mood disorders and osteoporosis, sphincter of Oddi constriction, exaggerated intracranial pressure elevation; seizure exacerbation (especially in children). Cardiac disorders: Bradycardia, palpitations, tachycardia. Ear and labyrinth disorders: Vertigo. Eye disorders: Miosis, blurred or double vision. Gastrointestinal disorders: Nausea, vomiting, abdominal cramps, abdominal pain, dry mouth, anorexia, gastrointestinal distress, pancreatitis. General disorders and administration site conditions: Malaise, tiredness, hypothermia. Hepatobiliary disorders: Biliary spasm. Musculoskeletal and connective tissue disorders: Uncontrolled muscle movements, muscle rigidity (after high doses). Nervous system disorders: Headache, dizziness, drowsiness. Psychiatric disorders: Sleep disturbances, confusion, restlessness, mental depression, hallucinations, nightmares, mood changes, euphoria, dysphoria. Renal and urinary disorders: Urinary retention, dysuria, ureteric spasm, micturition difficulty, antidiuretic effect. Reproductive system and breast disorders: Sexual dysfunction, erectile dysfunction, decreased libido. Respiratory, thoracic and mediastinal disorders: Dyspnoea. Skin and subcutaneous tissue disorders: Allergic reactions (e.g. skin rashes, urticaria, pruritus, sweating, facial oedema). Vascular disorders: Flushing, hypotension. Potentially Fatal: Respiratory depression; opioid addiction, abuse, and misuse; neonatal opioid withdrawal syndrome (prolonged use during pregnancy).
This drug may cause sedation and changes in vision (e.g. blurred or double vision), if affected, do not drive or operate machinery.
Chỉ số theo dõi
Monitor pain relief, bowel function, blood pressure, heart rate, and respiratory and mental status. Assess for signs and symptoms of substance abuse, misuse, or addiction; hypogonadism or hypoadrenalism.
Quá liều
Symptoms: Nausea, vomiting, constipation, lack of appetite, constricted pupils, confusion, somnolence progressing to stupor or coma, marked mydriasis with hypoxia, skeletal muscle flaccidity, cold and clammy skin, pulmonary oedema, bradycardia, hypotension, atypical snoring, partial or complete airway obstruction, and respiratory depression. Management: Symptomatic and supportive treatment. Ensure clear airway and institute assisted or controlled ventilation, if necessary. Empty the stomach by aspiration or lavage. May administer activated charcoal within 1 hour of ingestion. Administer naloxone if clinically significant respiratory or cardiac depression is present.
Tương tác
May increase CNS depression, respiratory depression, and/or hypotension with antihistamines and sodium oxybate. Delayed absorption of mexiletine. Antagonised gastrointestinal effect of cisapride and anti-emetics (e.g. domperidone, metoclopramide). Cimetidine may increase the plasma concentration of codeine. May enhance the risk of severe constipation with anticholinergics and anti-diarrhoeals. Decreased plasma concentration of active metabolites with CYP3A4 inducers (e.g. carbamazepine, phenytoin, rifampicin). Increased plasma concentration of active metabolites with CYP3A4 inhibitors (e.g. erythromycin, ketoconazole, ritonavir). Decreased therapeutic effect with CYP2D6 inhibitors (e.g. amiodarone, quinidine). Potentially Fatal: Severe CNS excitation or depression with MAOIs. Increased risk of sedation, respiratory depression, and coma with sedative agents including benzodiazepines or other CNS depressants (e.g. non-benzodiazepine sedatives or hypnotics, antipsychotics, anxiolytics, general anaesthetics, muscle relaxants, tranquillisers, and other opioids).
Tương tác với thức ăn
Enhanced hypotensive, sedative, and respiratory effects of alcohol.
Ảnh hưởng đến kết quả xét nghiệm
May interfere with gastric emptying studies and with hepatobiliary imaging using technetium Tc 99m disofenin.
Tác dụng
Description: Mechanism of Action: Codeine, a phenanthrene derivative, is an opioid agonist. Its analgesic property has been speculated to come from its conversion to morphine; it primarily binds to the μ-opioid receptor distributed throughout the CNS, but with a much weaker affinity than morphine. Its exact mechanism in cough suppression is unclear but it appears to have direct central action in the medulla. Additionally, it decreases intestinal motility through local and central mechanisms of action. Onset: 0.5-1 hour. Duration: 4-6 hours. Pharmacokinetics: Absorption: Well absorbed from the gastrointestinal tract. Bioavailability: 53%. Time to peak plasma concentration: 1 hour. Distribution: Crosses the placenta and enters breast milk. Volume of distribution: Approx 3-6 L/kg. Plasma protein binding: Approx 7-25%. Metabolism: Metabolised in the liver by UGT2B7 and UGT2B4 to codeine-6-glucuronide, by CYP2D6 to morphine (active), and by CYP3A4 to norcodeine. The active metabolite is further metabolised via glucuronidation to morphine-3-glucuronide and morphine-6-glucuronide (active). Excretion: Via urine (approx 90%; approx 10% as unchanged drug); faeces. Elimination half-life: Approx 3 hours.
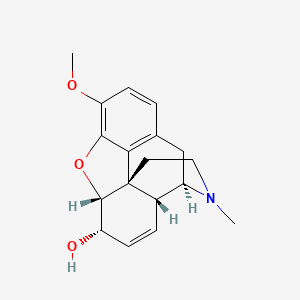
Đặc tính
Codeine Source: National Center for Biotechnology Information. PubChem Compound Summary for CID 5284371, Codeine. https://pubchem.ncbi.nlm.nih.gov/compound/Codeine. Accessed Mar. 25, 2024.
Bảo quản
Tab/Oral solution: Store between 15-30°C. Protect from light. Protect the tab from moisture.



 Đăng xuất
Đăng xuất