Adult: 2.4 g 4 hrly. Max: 18 g/day in meningococcal meningitis. Doses >1.2 g should be given at a rate not more than 300 mg/min. Child: Newborn infants: 100 mg/kg daily in 2 divided doses; 1-4 wk 150 mg/kg daily in 3 divided doses; >1 mth to 12 yr 180-300 mg/kg daily in 4-6 divided doses.
Parenteral Susceptible infections
Adult: 0.6-3.6 g daily in 4-6 divided doses, via IM, slow IV inj or infusion. Higher doses may be needed in more serious infections. IV doses >1.2 g should be given at a rate not more than 300 mg/min. Child: Newborn infants: 50 mg/kg daily in 2 divided doses; 1-4 wk 75 mg/kg daily in 3 divided doses; >1 mth to 12 yr 100 mg/kg daily in divided doses, not exceeding 4 g/day.
Renal Impairment
Dosing interval should be no more frequent than every 8-10 hr.
Administration
Should be taken on an empty stomach. Take w/ a full glass of water on an empty stomach 1 hr before or 2 hr after meals. Do not take acidic beverages w/in 1 hr of a dose.
Reconstitution
Loosen the powd, then, hold the vial horizontally and rotate it while slowly directing the stream of diluent against the wall of the vial. Shake the vial vigorously after all the diluent has been added. Depending on the route of admin, reconstitute w/ sterile water for inj, NaCl 0.9% inj or dextrose 5% inj.
Incompatibility
Amphotericin B, cimetidine, cytarabine, flucloxacillin, hydroxyzine, methylprednisolone, promethazine, metoclopramide and soln containing metal ions.
Contraindications
Hypersensitivity to benzylpenicillin and other penicillins.
Special Precautions
Patient w/ history of allergy esp β-lactam allergy and/or asthma, seizure disorder. Diabetic patients. Renal impairment. Pregnancy and lactation.
Monitor electrolyte, hepatic, renal, cardiac and haematologic function; signs and symptoms of anaphylaxis during 1st dose.
Overdosage
Symptoms: Agitation, confusion, asterixis, hallucinations, stupor, coma, multifocal myoclonus, seizures and encephalopathy, hyperkalaemia. Management: Symptomatic and supportive treatment.
Drug Interactions
May reduce the efficacy of OC. May increase the risk of methotrexate toxicity. Increased plasma concentration w/ probenecid. Antagonism of bactericidal effect w/ bacteriostatic antibacterials (e.g. erythromycin, tetracyclines).
Food Interaction
Food may reduce the absorption of benzylpenicillin.
Lab Interference
May interfere w/ urinary glucose tests, Coombs test, and test for urinary or serum proteins. May interfere w/ diagnostic tests which use bacteria (e.g. Guthrie test).
Action
Description: Benzylpenicillin has a bactericidal action against gm+ve bacteria, gm-ve cocci, some other gm-ve bacteria, spirochetes and actinomycetes. It inhibits final cross-linking stage of peptidoglycan production through binding and inactivation of transpeptidases on the inner surface of the bacterial cell membrane thus inhibiting bacterial cell wall synthesis. It is inhibited by penicillinase and other β-lactamases. Pharmacokinetics: Absorption: Rapidly appears in blood after IM inj. Inactivated fairly rapidly by gastric acid and up to approx 30% is absorbed. Absorption is reduced by the presence of food. Time to peak plasma concentration: 15-30 min (IM); approx 1 hr (oral/IV). Distribution: Widely distributed. Crosses the placenta and enters breast milk (small amounts). Volume of distribution: 0.53-0.67 L/kg. Plasma protein binding: Approx 60%. Metabolism: Undergoes limited hepatic metabolism to penicilloic acid. Excretion: Via urine (58-85% as unchanged drug) and bile (small amounts). Plasma half-life: Approx 30 min.
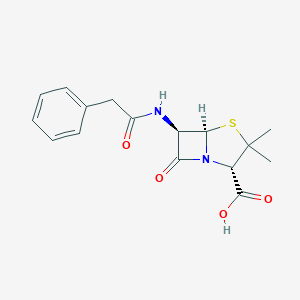
Chemical Structure
Benzylpenicillin Source: National Center for Biotechnology Information. PubChem Database. Penicillin g, CID=5904, https://pubchem.ncbi.nlm.nih.gov/compound/Penicillin-g (accessed on Jan. 21, 2020)
Storage
Store between 20-25°C. Reconstituted soln: Store between 2-8°C.
Anon. Penicillin G (Parenteral). Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 26/06/2014.Buckingham R (ed). Benzylpenicillin. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 25/06/2014.McEvoy GK, Snow EK, Miller J et al (eds). Penicillin G Potassium, Penicillin G Sodium. AHFS Drug Information (AHFS DI) [online]. American Society of Health-System Pharmacists (ASHP). https://www.medicinescomplete.com. Accessed 26/06/2014.Pfizerpen Powder for solution (Roerig). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 26/06/2014.



 Sign Out
Sign Out