Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Hypercalcemia of Malignancy: The maximum recommended dose of Zoledronic acid in hypercalcemia of malignancy (albumin-corrected serum calcium ≥ 12 mg/dl [3.0 mmol/L]) is 4 mg. The 4-mg dose must be given as a single-dose intravenous infusion over no less than 15 minutes. Patients who receive Zoledronic acid should have serum creatinine assessed prior to each treatment.
Dose adjustments of Zoledronic acid are not necessary in treating patients for hypercalcemia of malignancy presenting with mild-to-moderate renal impairment prior to initiation of therapy (serum creatinine <400 μmol/L or <4.5 mg/dL). Patients should be adequately rehydrated prior to administration of Zoledronic acid. Consideration should be given to the severity of, as well as the symptoms of, tumor-induced hypercalcemia when considering use of Zoledronic acid. Vigorous saline hydration, an integral part of hypercalcemia therapy, should be initiated promptly and an attempt should be made to restore the urine output to about 2 L/day throughout treatment. Mild or asymptomatic hypercalcemia may be treated with conservative measures (i.e., saline hydration, with or without loop diuretics). Patients should be hydrated adequately throughout the treatment, but overhydration, especially in those patients who have cardiac failure, must be avoided. Diuretic therapy should not be employed prior to correction of hypovolemia. Retreatment with Zoledronic acid 4 mg may be considered if serum calcium does not return to normal or remain normal after initial treatment. It is recommended that a minimum of 7 days elapse before retreatment, to allow for full response to the initial dose. Renal function must be carefully monitored in all patients receiving Zoledronic acid and serum creatinine must be assessed prior to retreatment with Zoledronic acid.
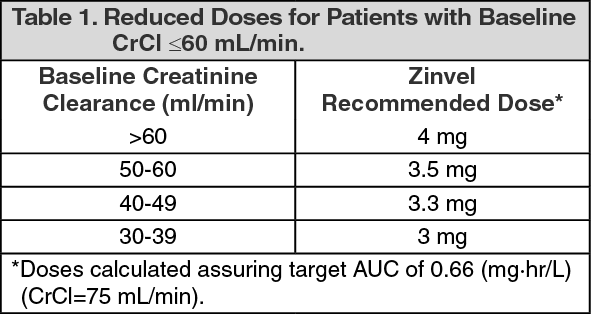
Multiple Myeloma and Metastatic Bone Lesions of Solid Tumors: The recommended dose of Zoledronic acid in patients with multiple myeloma and metastatic bone lesions from solid tumors for patients with creatinine clearance >60 mL/min is 4 mg infused over no less than 15 minutes every 3-4 weeks. The optimal duration of therapy is not known. Upon treatment initiation, the recommended Zoledronic acid doses for patients with reduced renal function (mild and moderate renal impairment) are listed in Table 1. These doses are calculated to achieve the same AUC as that achieved in patients with creatinine clearance of 75 mL/min. Creatinine clearance (CrCl) is calculated using the Cockcroft-Gault formula. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
During treatment, serum creatinine should be measured before each Zoledronic acid dose and treatment should be withheld for renal deterioration. In the clinical studies, renal deterioration was defined as follows: For patients with normal baseline creatinine, increase of 0.5 mg/dL.
For patients with abnormal baseline creatinine, increase of 1.0 mg/dL.
In the clinical studies, Zoledronic acid treatment was resumed only when the creatinine returned to within 10% of the baseline value. Zoledronic acid should be reinitiated at the same dose as that prior to treatment interruption.
Patients should also be administered an oral calcium supplement of 500 mg and a multiple vitamin containing 400 IU of Vitamin D daily.
Preparation of Solution: 4 mg Dose: Vials of Zoledronic acid concentrate for infusion contain overfill allowing for the withdrawal of 5 mL of concentrate (equivalent to 4 mg zoledronic acid). This concentrate should immediately be diluted in 100 mL of sterile 0.9% Sodium Chloride, USP, or 5% Dextrose Injection, USP. Do not store undiluted concentrate in a syringe, to avoid inadvertent injection.
Preparing Reduced Doses for Patients with Baseline CrCl ≤ 60 mL/min: Withdraw the appropriate volume of the Zoledronic acid concentrate from the vial for the dose required (see Table 2).
Click on icon to see table/diagram/image
The withdrawn concentrate must be diluted in 100 mL of sterile 0.9% Sodium Chloride, USP, or 5% Dextrose Injection, USP.
For All Prepared Doses: If not used immediately after dilution with infusion media, for microbiological integrity, the solution should be refrigerated at 2°C-8°C (36°F-46°F). The refrigerated solution should then be equilibrated to room temperature prior to administration. The total time between dilution, storage in the refrigerator, and end of administration must not exceed 24 hours.
Zoledronic acid must not be mixed with calcium or other divalent cation-containing infusion solutions, such as Lactated Ringer's solution, and should be administered as a single intravenous solution in a line separate from all other drugs.
Method of Administration: Due to the risk of clinically significant deterioration in renal function, which may progress to renal failure, single doses of Zoledronic acid should not exceed 4 mg and the duration of infusion should be no less than 15 minutes.



 Sign Out
Sign Out