Pharmacology: Pharmacodynamics: Mechanism of action: Bortezomib is a reversible inhibitor of the chymotrypsin-like activity of the 26S proteasome in mammalian cells. The 26S proteasome is a large protein complex that degrades ubiquitinated proteins. The ubiquitin-proteasome pathway plays an essential role in regulating the intracellular concentration of specific proteins, thereby maintaining homeostasis within cells. Inhibition of the 26S proteasome prevents this targeted proteolysis which can affect multiple signaling cascades within the cell. This disruption of normal homeostatic mechanisms can lead to cell death. Experiments have demonstrated that bortezomib is cytotoxic to a variety of cancer cell types
in vitro. Bortezomib causes a delay in tumor growth
in vivo in nonclinical tumor models, including multiple myeloma.
Data from
in vitro,
ex-vivo, and animal models with bortezomib suggest that it increases osteoblast differentiation and activity and inhibits osteoclast function. These effects have been observed in patients with multiple myeloma affected by an advanced osteolytic disease and treated with bortezomib.
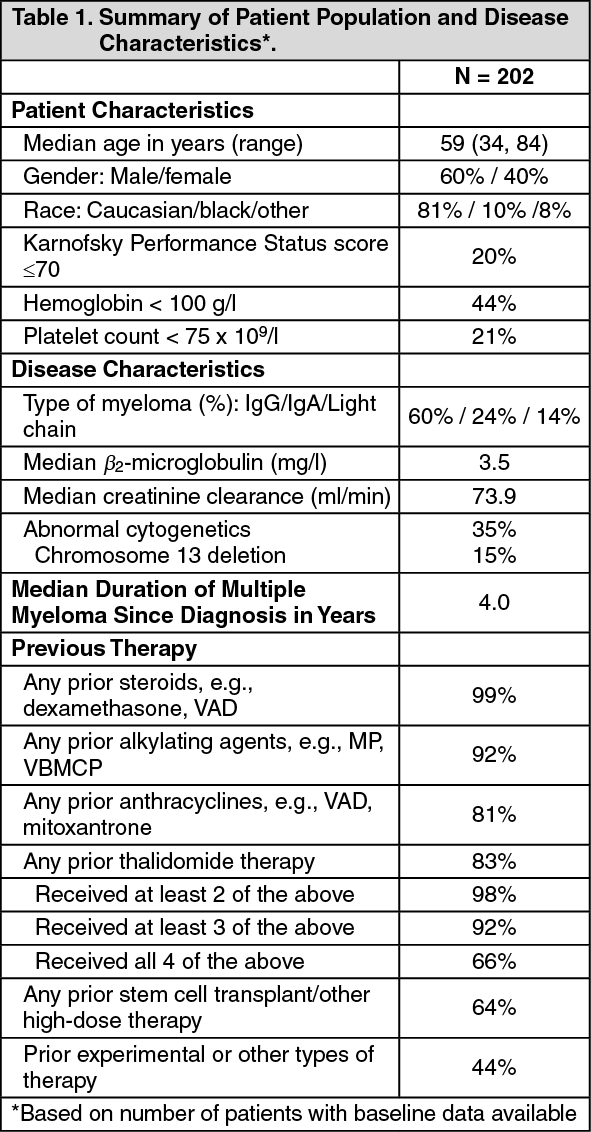
Clinical Trials: Phase 2 Clinical Studies in Relapsed Multiple Myeloma: The safety and efficacy of VELCADE IV were evaluated in an open-label, single-arm, multicenter study of 202 patients who had received at least 2 prior therapies and demonstrated disease progression on their most recent therapy. The median number of prior therapies was six. Baseline patient and disease characteristics are summarized in Table 1.
An IV bolus injection of VELCADE 1.3 mg/m
2/dose was administered twice weekly for 2 weeks, followed by a 10 day rest period (21 day treatment cycle) for a maximum of 8 treatment cycles. The study employed dose modifications for toxicity (see Dosage & Administration). Patients who experienced a response to VELCADE treatment were allowed to continue VELCADE treatment in an extension study. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
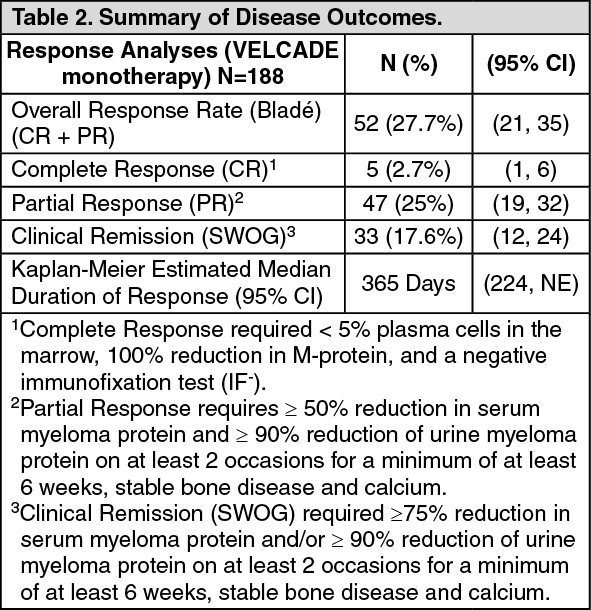
Responses to VELCADE alone are shown in Table 2. Response rates to VELCADE alone were determined by an independent review committee (IRC) based on criteria published by Bladé and others. Complete response required <5% plasma cells in the marrow, 100% reduction in M protein, and a negative immunofixation test (IF-). Response rates using the SWOG criteria are also shown. SWOG response required a ≥75% reduction in serum myeloma protein and/or ≥90% urine protein.3 A total of 188 patients were evaluated for response; 9 patients with nonmeasurable disease could not be evaluated for response by the IRC. Five patients were excluded from the efficacy analyses because they had minimal prior therapy.
Ninety-eight percent of study patients received a starting dose of 1.3 mg/m
2 administered IV. Twenty-eight percent of these patients received a dose of 1.3 mg/m
2 throughout the study, while 33% of patients who started at a dose of 1.3 mg/m
2 had to have their dose reduced during the study. Sixty-three percent of patients had at least one dose held during the study. In general, patients who had a confirmed CR received 2 additional cycles of VELCADE treatment beyond confirmation. It was recommended that responding patients receive up to 8 cycles of VELCADE therapy. The mean number of cycles administered was 6.
The median time to response was 38 days (range 30 to 127 days).
The median survival of all patients enrolled was 16 months (range <1 to 18+ months). (See Table 2.)
Click on icon to see table/diagram/image
In this study, the response rate to VELCADE was independent of the number and types of prior therapies. There was a decreased likelihood of response in patients with either >50% plasma cells or abnormal cytogenetics in the bone marrow. Responses were seen in patients with chromosome 13 abnormalities.
A small dose-response study (M34100-24) was performed in 54 patients with multiple myeloma who received a 1.0 mg/m
2/dose or a 1.3 mg/m
2/dose twice weekly for two out of three weeks. A single complete response was seen at each dose, and there were overall (CR + PR) response rates of 30% (8/27) at 1.0 mg/m
2 and 38% (10/26) at 1.3 mg/m
2.
Patients who did not obtain an optimal response to therapy with VELCADE alone (progressive or stable disease after 2 or 4 cycles, respectively) were able to receive high-dose dexamethasone in conjunction with VELCADE (i.e., 40 mg dexamethasone with each dose of VELCADE administered orally as 20 mg on the day of and 20 mg the day after VELCADE administration, (i.e., Days 1, 2, 4, 5, 8, 9, 11, and 12), thus 160 mg over 3 weeks). A total of 74 patients were administered dexamethasone in combination with VELCADE and were assessed for response. Eighteen percent (13/74) of patients achieved or had an improved response (CR 11% or PR 7%) with combination treatment.
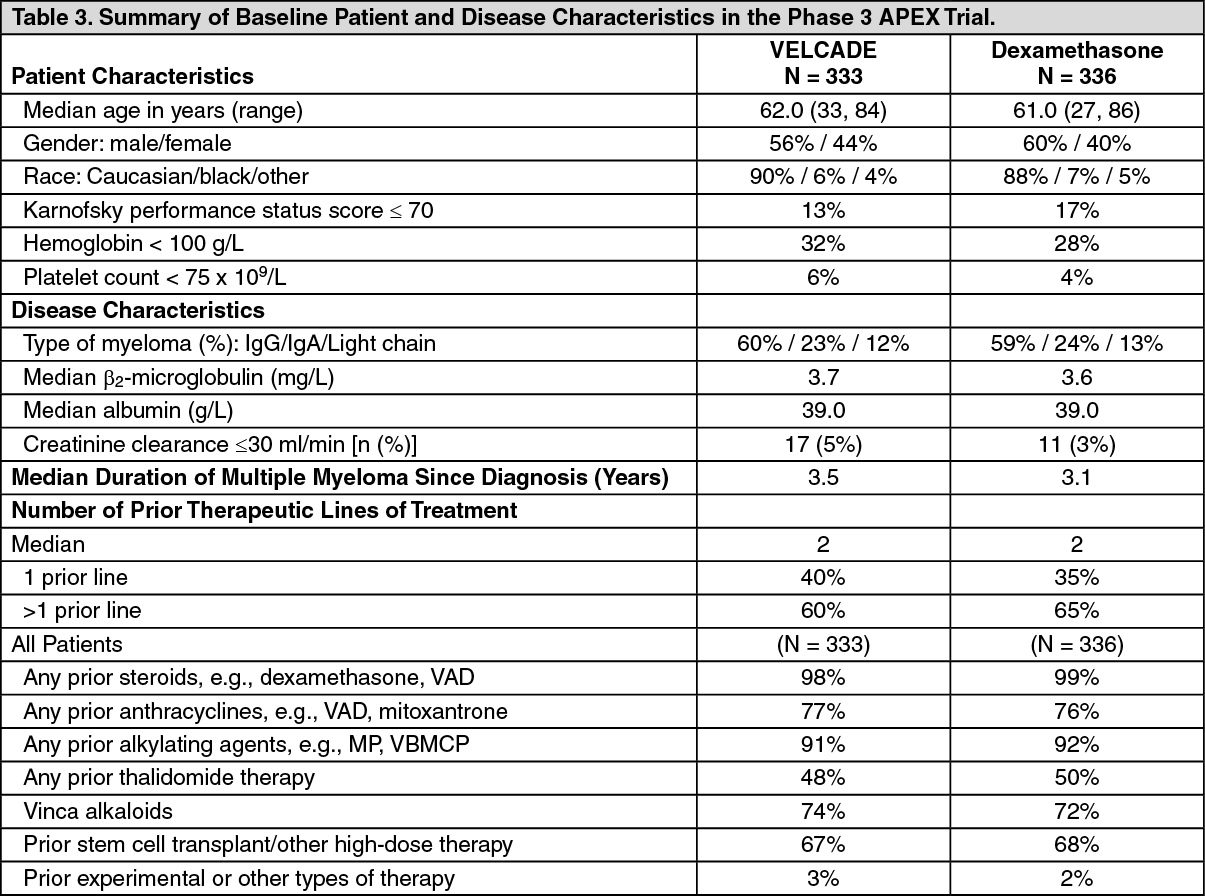
Randomized, Open-Label Clinical Study in Relapsed Multiple Myeloma comparing VELCADE to Dexamethasone: A prospective phase 3, international, randomized (1:1), stratified, open-label clinical trial [M34101-039 (APEX)] enrolling 669 patients was designed to determine whether VELCADE resulted in improvement in time to progression (TTP) compared to high-dose dexamethasone in patients with progressive multiple myeloma following 1 to 3 prior therapies. Patients considered to be refractory to prior high-dose dexamethasone were excluded as were those with baseline grade ≥2 peripheral neuropathy or platelet counts <50,000/µl. A total of 627 patients were evaluable for response.
Stratification factors were based on the number of lines of prior therapy the patient had previously received (1 previous line versus more than 1 line of therapy), time of progression relative to prior treatment (progression during or within 6 months of stopping their most recent therapy versus relapse >6 months after receiving their most recent therapy), and screening β
2-microglobulin levels (≤ 2.5 mg/l versus >2.5 mg/l).
Baseline patient and disease characteristics are summarized in Table 3.
Click on icon to see table/diagram/image
Patients in the VELCADE treatment group were to receive eight 3-week treatment cycles followed by three 5-week treatment cycles of VELCADE. Within each 3-week treatment cycle, VELCADE 1.3 mg/m
2/dose alone was administered by IV bolus twice weekly for 2 weeks on Days 1, 4, 8, and 11 followed by a 10-day rest period (Days 12 to 21). Within each 5-week treatment cycle, VELCADE 1.3 mg/m
2/dose alone was administered by IV bolus once weekly for 4 weeks on Days 1, 8, 15, and 22 followed by a 13-day rest period (Days 23 to 35) (see Dosage & Administration).
Patients in the dexamethasone treatment group were to receive four 5-week treatment cycles followed by five 4-week treatment cycles. Within each 5-week treatment cycle, dexamethasone 40 mg/day PO was administered once daily on Days 1 to 4, 9 to 12, and 17 to 20 followed by a 15-day rest period (Days 21 to -35). Within each 4-week treatment cycle, dexamethasone 40 mg/day PO was administered once daily on Days 1 to 4 followed by a 24-day rest period (Days 5 to 28). Patients with documented progressive disease on dexamethasone were offered VELCADE at a standard dose and schedule on a companion study.
Following a preplanned interim analysis of time to progression, the dexamethasone arm was halted and all patients randomized to dexamethasone were offered VELCADE, regardless of disease status. At this time of study termination, a final statistical analysis was performed. Due to this early termination of the study, the median duration of follow-up for surviving patients (n=534) is limited to 8.3 months.
In the VELCADE arm, 34% of patients received at least 1 VELCADE dose in all 8 of the 3-week cycles of therapy, and 13% received at least 1 dose in all 11 cycles. The average number of VELCADE doses during the study was 22, with a range of 1 to 44. In the dexamethasone arm, 40% of patients received at least 1 dose in all 4 of the 5-week treatment cycles of therapy, and 6% received at least 1 dose in all 9 cycles.
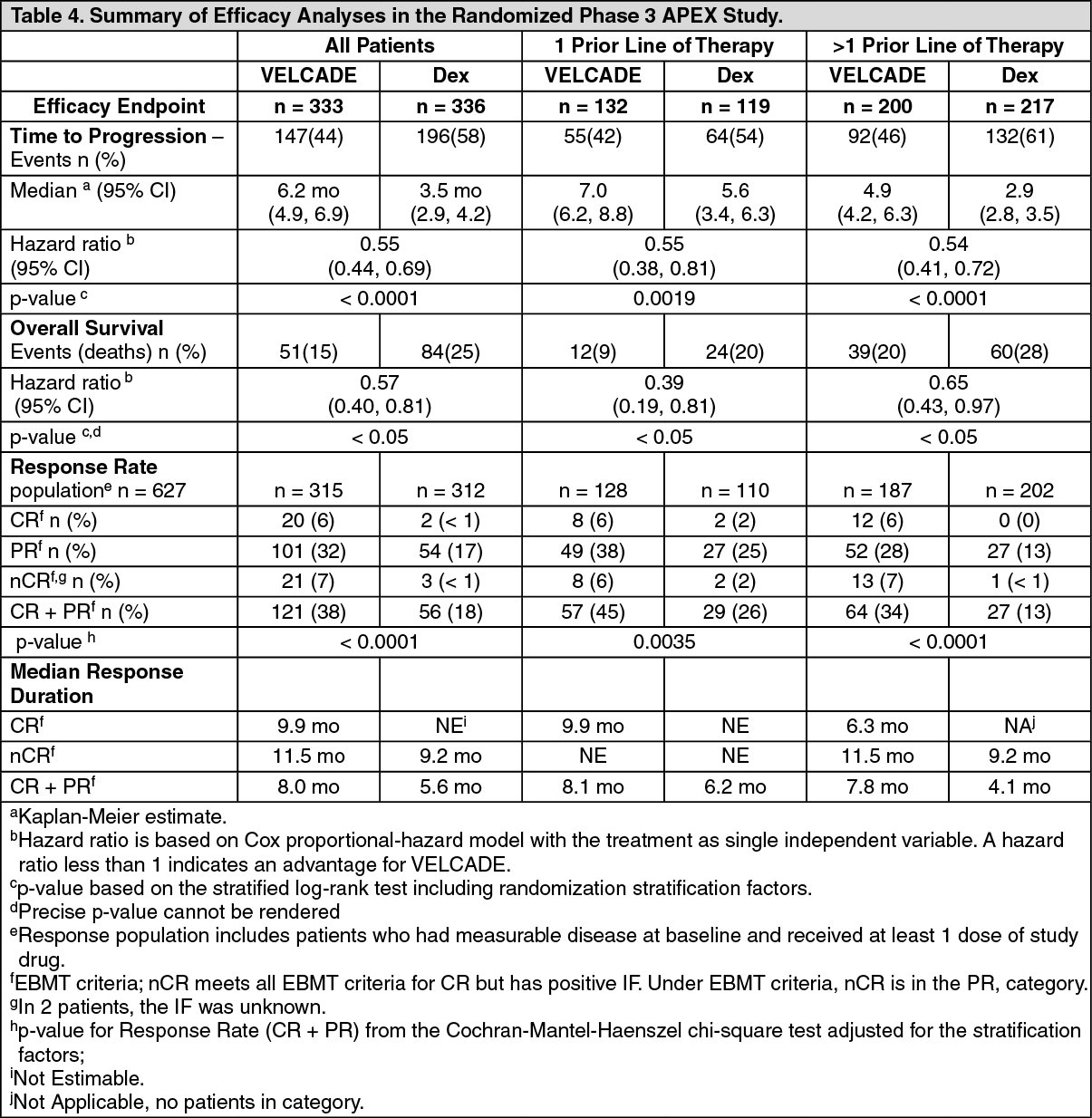
The time to event analyses and response rates from the phase 3 trial are presented in Table 4. Response and progression were assessed using the European Group for Blood and Marrow Transplantation (EBMT) criteria. Complete response (CR) required <5% plasma cells in the marrow, 100% reduction in M-protein, and a negative immunofixation test (IF-). Partial Response (PR) requires ≥50% reduction in serum myeloma protein and ≥90% reduction of urine myeloma protein on at least 2 occasions for a minimum of at least 6 weeks along with stable bone disease and normal calcium. Near complete response (nCR) was defined as meeting all the criteria for complete response including 100% reduction in M-protein by protein electrophoresis, however M-protein was still detectable by immunofixation (IF
+). (See Table 4.)
Click on icon to see table/diagram/image
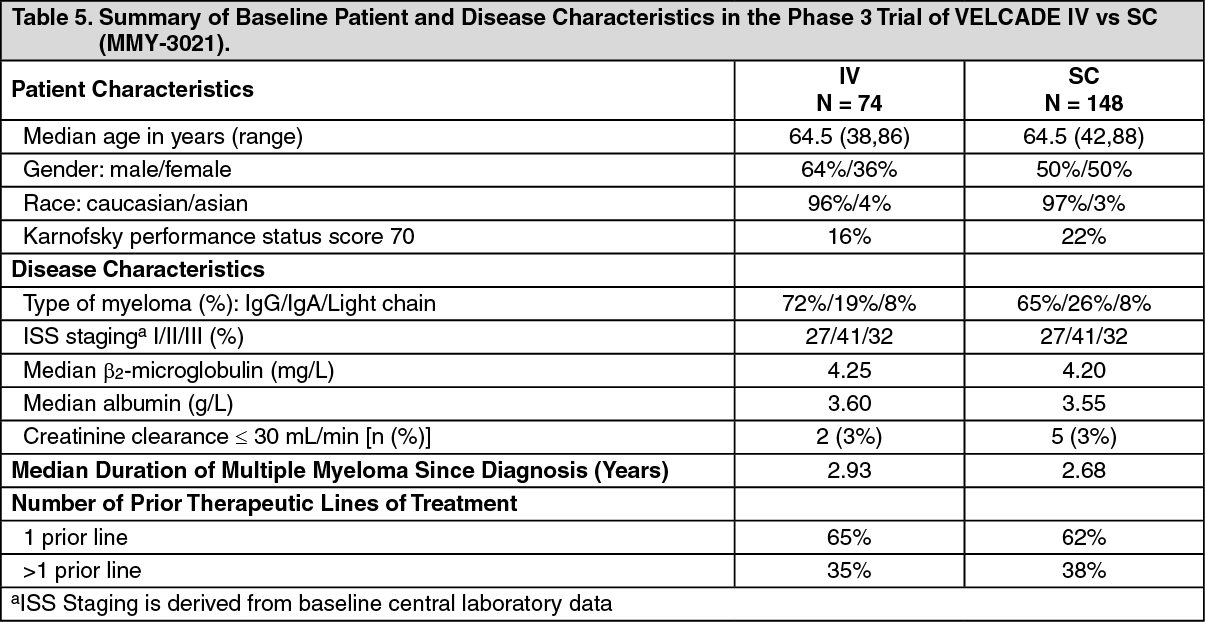
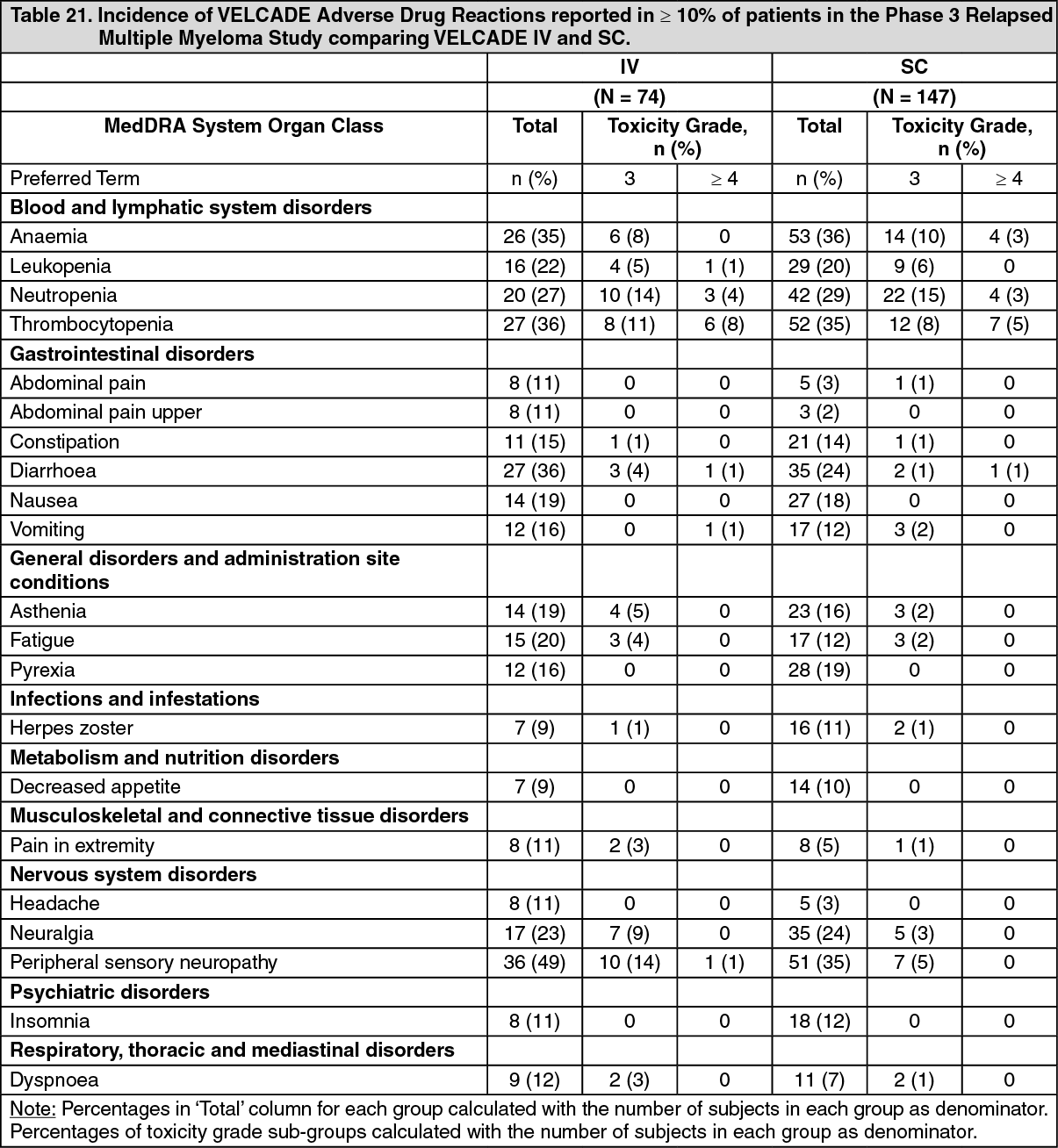
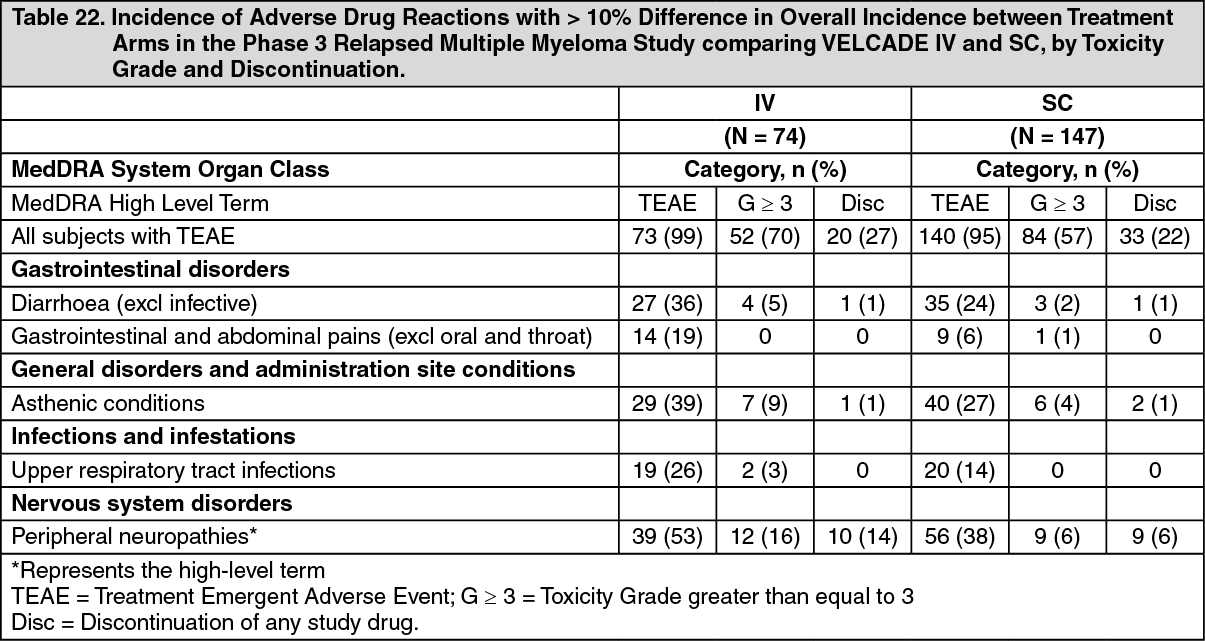
Randomized, Open-Label Clinical Study in Relapsed Multiple Myeloma comparing VELCADE IV and SC: An open label, randomized, phase 3 non-inferiority study (MMY-3021) compared the efficacy and safety of the subcutaneous administration (SC) of VELCADE versus the intravenous administration (IV). This study included 222 patients with relapsed multiple myeloma, who were randomized in a 2:1 ratio to receive 1.3 mg/m
2 of VELCADE by either the SC or IV route for 8 cycles. Patients who did not obtain an optimal response (less than Complete Response (CR)) to therapy with VELCADE alone after 4 cycles were allowed to receive dexamethasone 20 mg daily on the day of and after VELCADE administration. Patients with baseline grade ≥2 peripheral neuropathy or platelet counts <50,000/µL were excluded. A total of 218 patients were evaluable for response.
Stratification factors were based on the number of lines of prior therapy the patient had received (1 previous line versus more than 1 line of therapy), and international staging system (ISS) stage (incorporating beta
2-microglobulin and albumin levels; Stages I, II, or III). Baseline patient and disease characteristics are summarized in Table 5.
Click on icon to see table/diagram/image
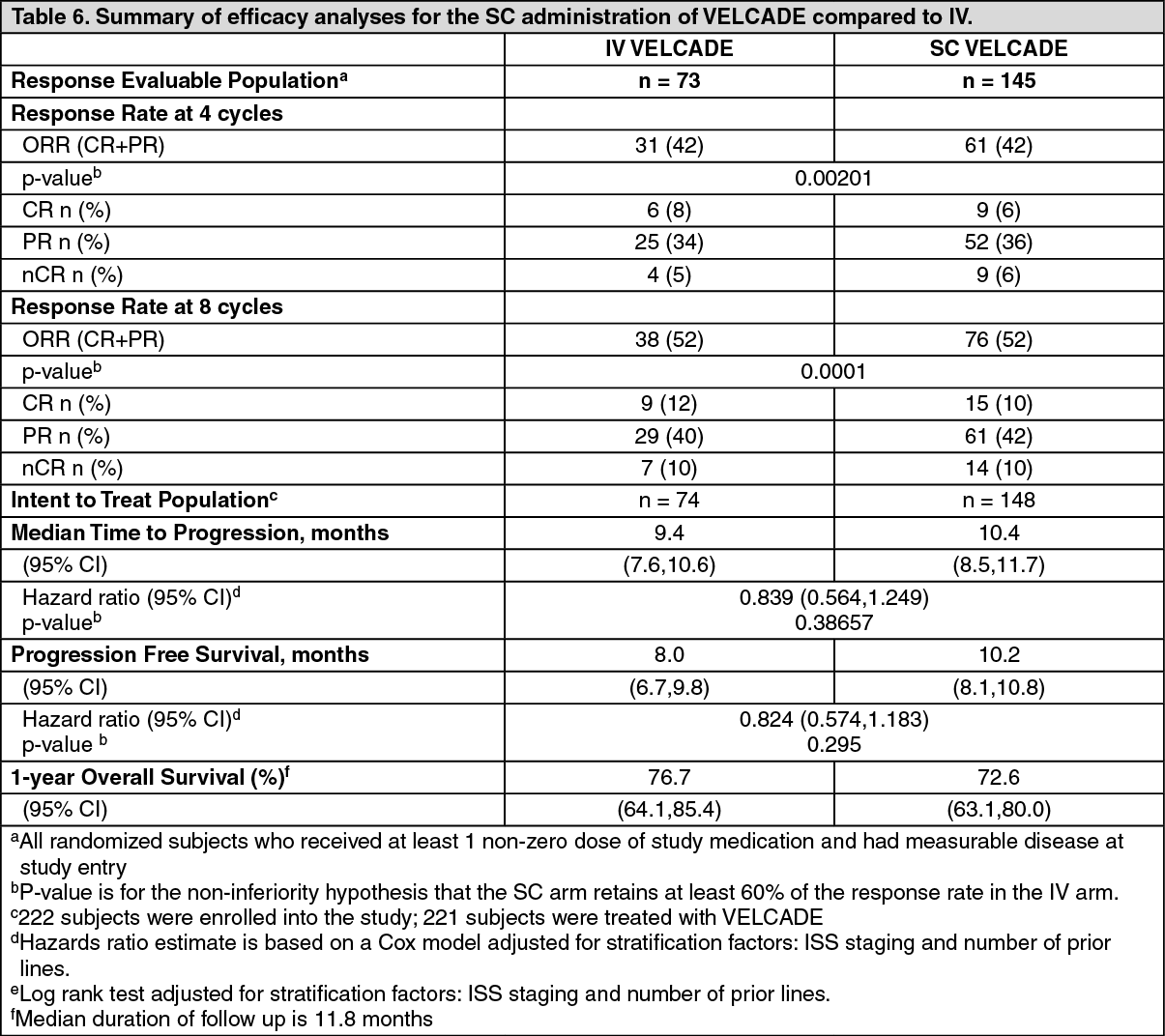
This study met its primary objective of non-inferiority for response rate (CR + PR) after 4 cycles of single agent VELCADE for both the SC and IV routes, 42% in both groups. In addition, secondary response-related and time to event related efficacy endpoints showed consistent results for SC and IV administration (see Table 6).
Click on icon to see table/diagram/image
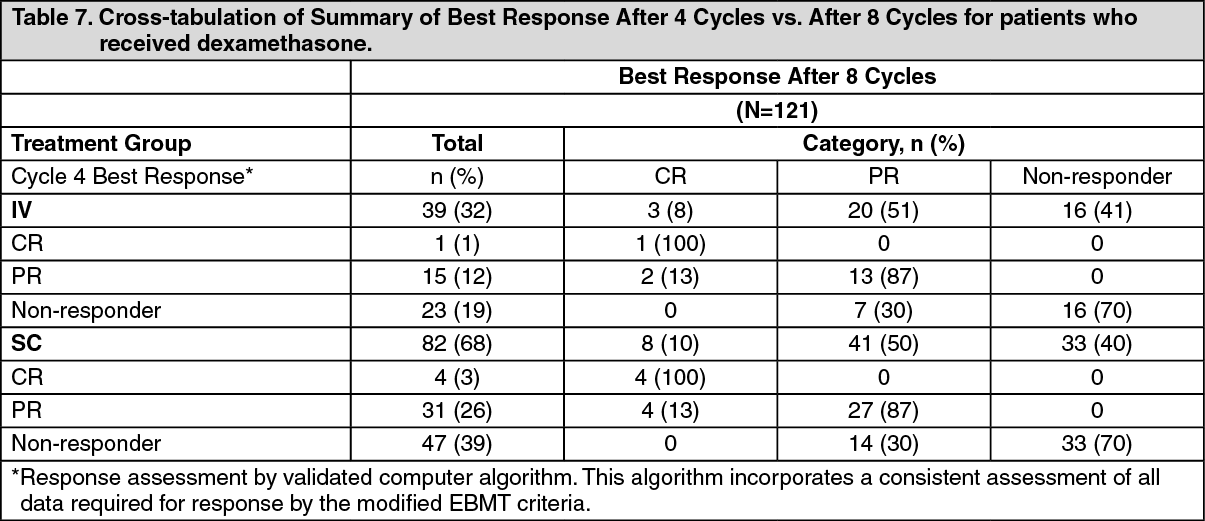
Table 7 presents a cross-tabulation summary of best response by algorithm after 4 cycles versus after 8 cycles for patients who received dexamethasone. Eighty-two subjects in the SC treatment group and 39 subjects in the IV treatment group received dexamethasone after cycle 4.
Dexamethasone had a similar effect on improvement of response on both treatment arms: 30% (SC) and 30% (IV) of patients with no response at end of Cycle 4 obtained a response later.
13% (SC) and 13% (IV) of patients with PR at end of Cycle 4 obtained a CR later. (See Table 7.)
Click on icon to see table/diagram/image
Relative to previously reported outcomes, the ORR after 8 cycles of treatment (52% in both treatment groups) and time to progression (median 10.4 months and 9.4 months in SC and IV treatment groups, respectively), including the effect of the addition of dexamethasone from cycle 5 onwards, were higher than observed in prior registration study with single agent IV VELCADE (38% ORR and median TTP of 6.2 months for the VELCADE arm). Time to Progression and ORR was also higher compared to the subgroup of patients that received only 1 prior line of therapy (43% ORR and median TTP of 7.0 months) (see Table 4).
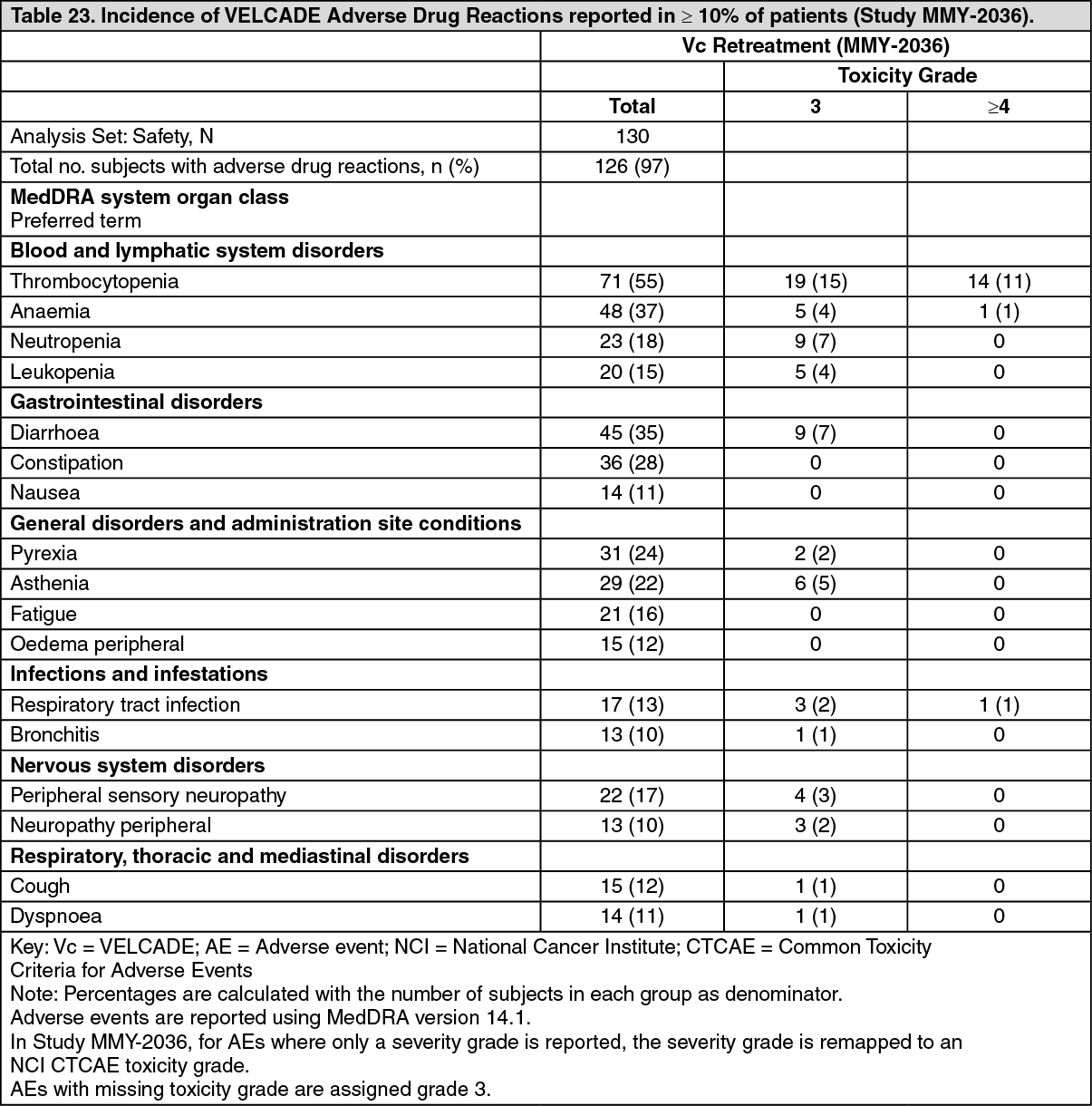
VELCADE Retreatment in Relapsed Multiple Myeloma: Study MMY-2036 (RETRIEVE) was an open label, multicenter study designed to determine the efficacy and safety of retreatment with VELCADE in 130 patients with relapsed multiple myeloma. Patients had previously tolerated 1.0 or 1.3 mg/m
2 VELCADE alone or in combination with other agents, had CR or PR upon completion of VELCADE therapy and subsequently relapsed.
As assessed by EBMT criteria, the primary endpoint of best response was achieved in 40% of patients who had a response of PR or better including 1% of whom had a best response of CR. In these 40% of patients (n=50) who had a best response of PR or better, the median time to progression (TTP) was 8.4 months (range: 3.3 to 20.7 months). The median duration of response in these patients was 6.5 months (range: 0.6 to 19.3 months).
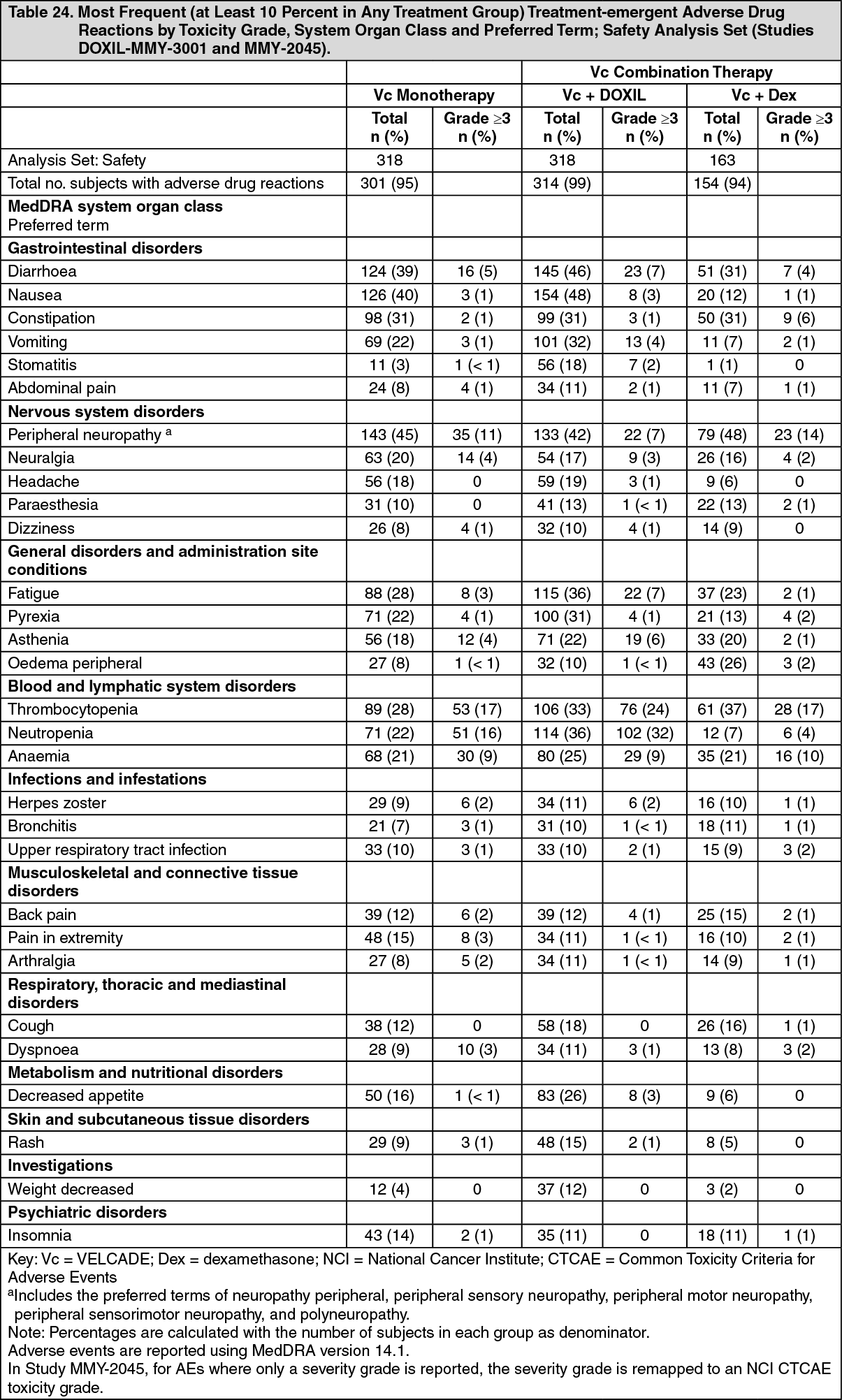
VELCADE Combination Treatment with Pegylated Liposomal Doxorubicin: A Phase 3 randomized, parallel-group, open-label, multicentre study (DOXIL-MMY-3001) was conducted in 646 patients comparing the safety and efficacy of VELCADE plus pegylated liposomal doxorubicin combination therapy with VELCADE monotherapy in patients with multiple myeloma who had received at least 1 prior therapy and who did not progress while receiving anthracycline-based therapy. The primary efficacy endpoint was TTP while the secondary efficacy endpoints were OS and ORR (CR+PR), using the European Group for Blood and Marrow Transplantation (EBMT) criteria.
There was a significant improvement in the primary endpoint of time to progression (TTP) for patients treated with combination therapy of VELCADE and pegylated liposomal doxorubicin. A protocol-defined interim analysis (based on 249 TTP events) triggered early study termination for efficacy. This interim analysis showed a TTP risk reduction of 45% (95% CI; 29-57%), p<0.0001. The median TTP was 6.5 months for the VELCADE monotherapy patients compared with 9.3 months for the VELCADE plus pegylated liposomal doxorubicin combination therapy patients. These results, though not mature, constituted the protocol defined final analysis.
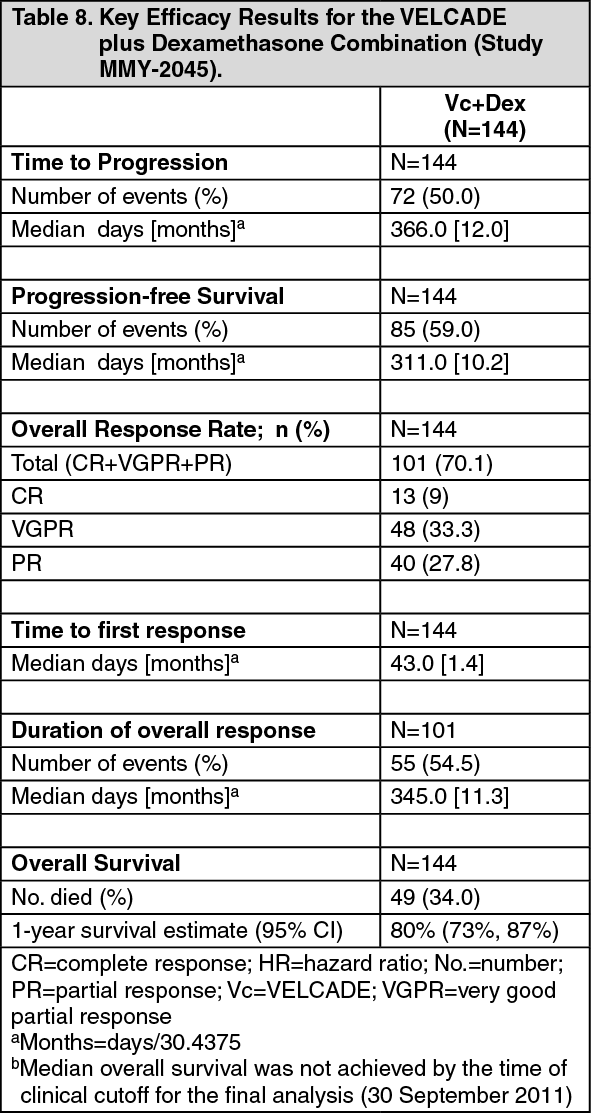
VELCADE Combination Treatment with Dexamethasone: Study MMY-2045 was a Phase 2 randomised open-label study to evaluate VELCADE in combination with dexamethasone (Vc+Dex) followed by either Vc+Dex or Vc+Dex in combination with cyclophosphamide (VDC), or lenalidomide (VDL). 163 patients with relapsed/progressive or refractory multiple myeloma were enrolled. The primary efficacy endpoint was the ORR. Secondary endpoints were changes in renal function after 4 cycles of Vc+Dex treatment, time to response, TTP, duration of response, PFS, 1-year survival, and OS.
The key efficacy results in 144 patients who received the VELCADE plus dexamethasone combination are presented in Table 8. The results demonstrate incremental benefit when compared to the previous, well-controlled VELCADE monotherapy study (APEX) and a positive effect of the combination of Vc+Dex on response rates, TTP, time to first response, PFS, and 1-year survival rate. The results are also consistent with Study MMY-3021 in which an improvement in response was seen when dexamethasone was added to VELCADE treatment in multiple myeloma patients after 4 cycles. (See Table 8.)
Click on icon to see table/diagram/image
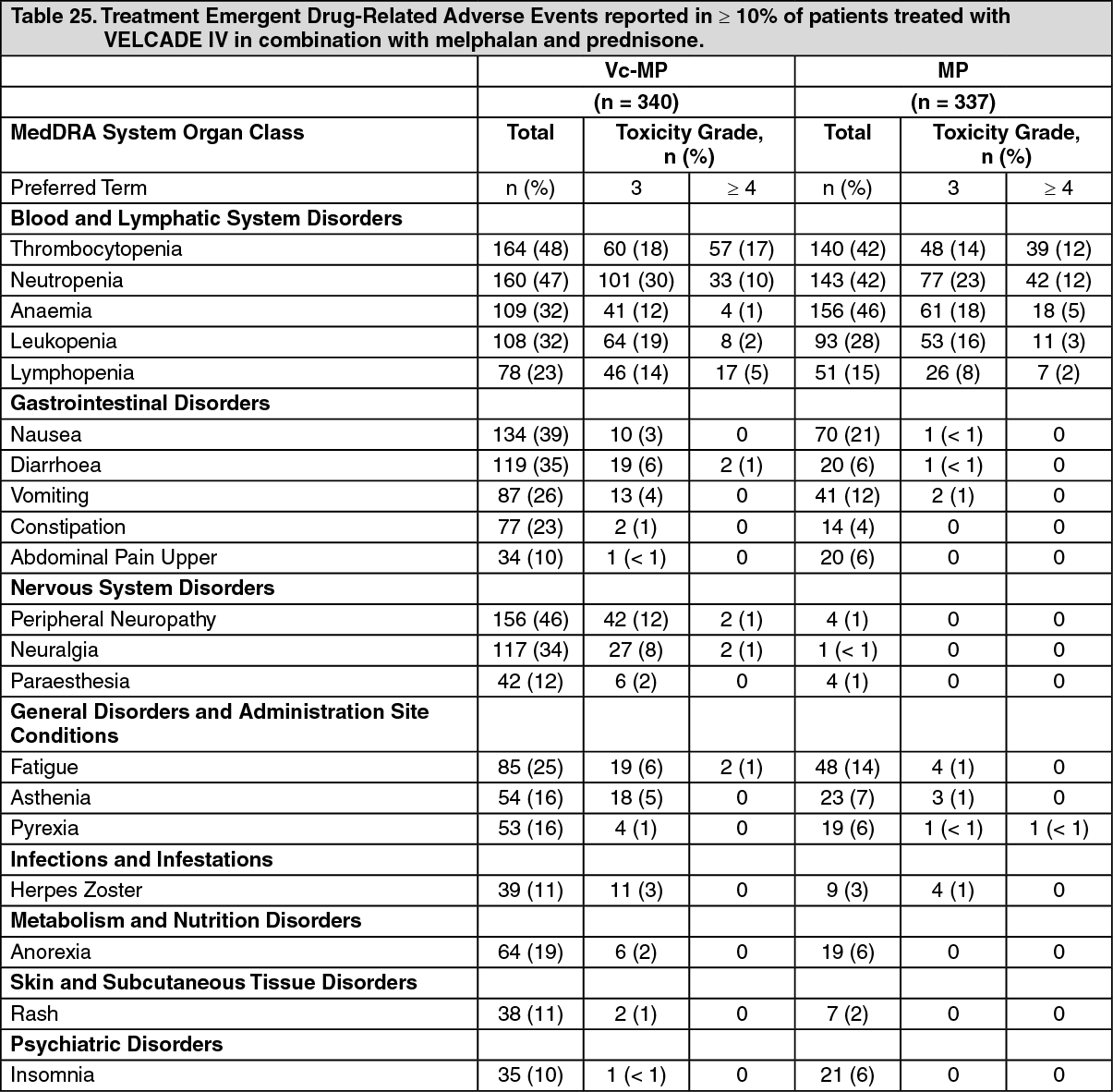
Randomized, Open-Label Clinical Study in Patients with Previously Untreated Multiple Myeloma: A prospective phase 3, international, randomized (1:1), open-label clinical study [MMY-3002 (VISTA)] of 682 patients was conducted to determine whether VELCADE (1.3 mg/m
2) in combination with melphalan (9 mg/m
2) and prednisone (60 mg/m
2) resulted in improvement in time to progression (TTP) when compared to melphalan (9 mg/m
2) and prednisone (60 mg/m
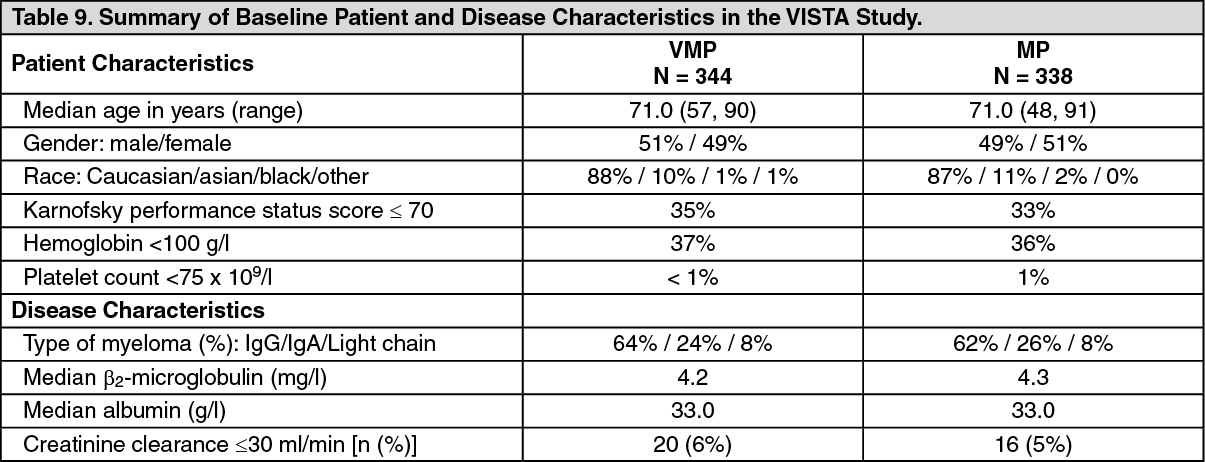
2) in patients with previously untreated multiple myeloma. This study included patients who were not candidates for stem-cell transplant. Treatment was administered for a maximum of 9 cycles (approximately 54 weeks) and was discontinued early for disease progression or unacceptable toxicity. Baseline demographics and patient characteristics are summarized in Table 9.
Click on icon to see table/diagram/image
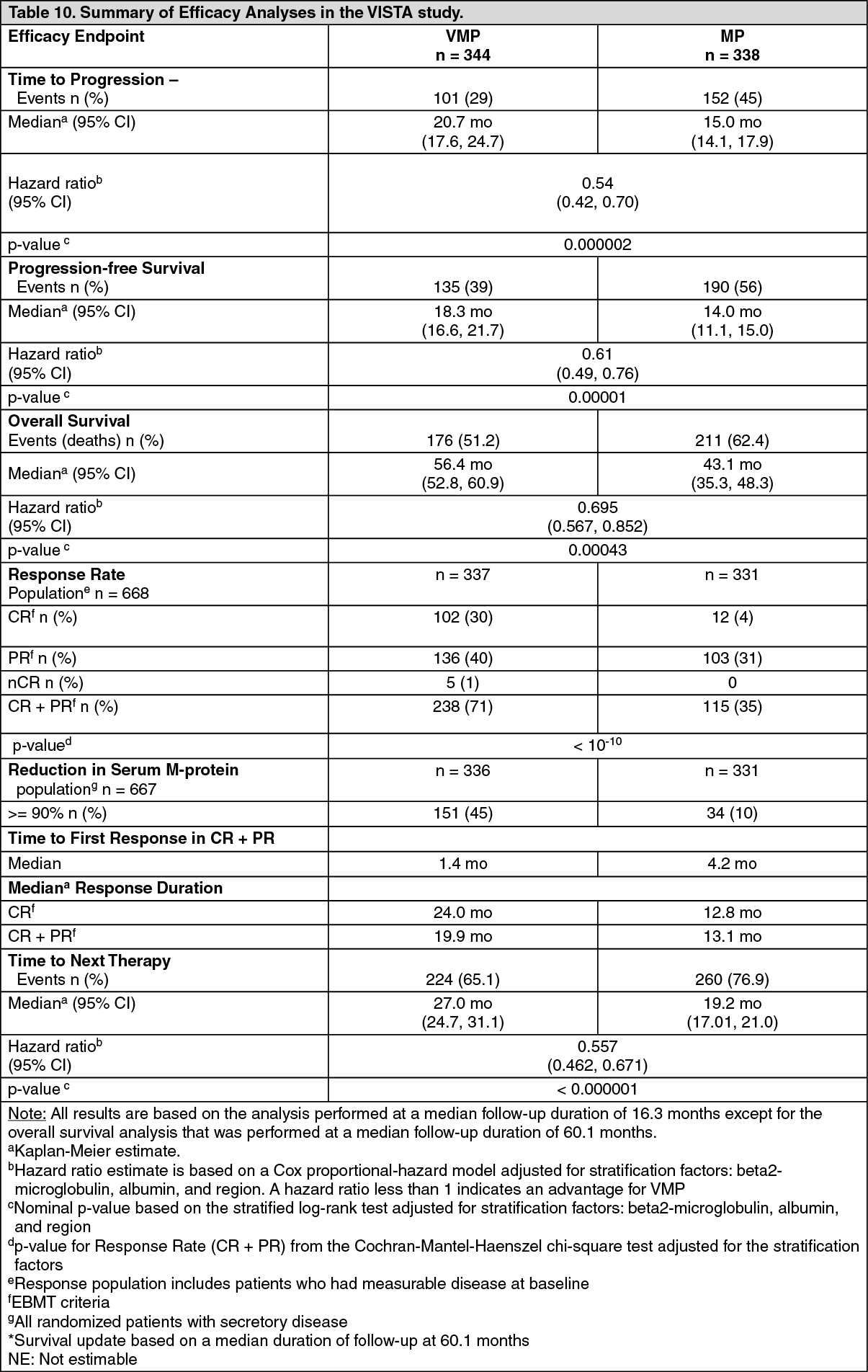
At the time of a pre-specified interim analysis, the primary endpoint, time to progression, was met and patients in the MP arm were offered VcMP treatment. Median follow-up was 16.3 months. The final survival update was performed with a median duration of follow-up at 60.1 months. A statistically significant survival benefit in favor of the VcMP treatment group was observed (HR=0.695; p=0.00043) despite subsequent therapies that included VELCADE based regimens. The median survival in MP treatment group has been estimated at 43.1 months, and the median survival on the VcMP treatment group has been estimated at 56.4 months . Efficacy results are presented in Table 10.
Click on icon to see table/diagram/image
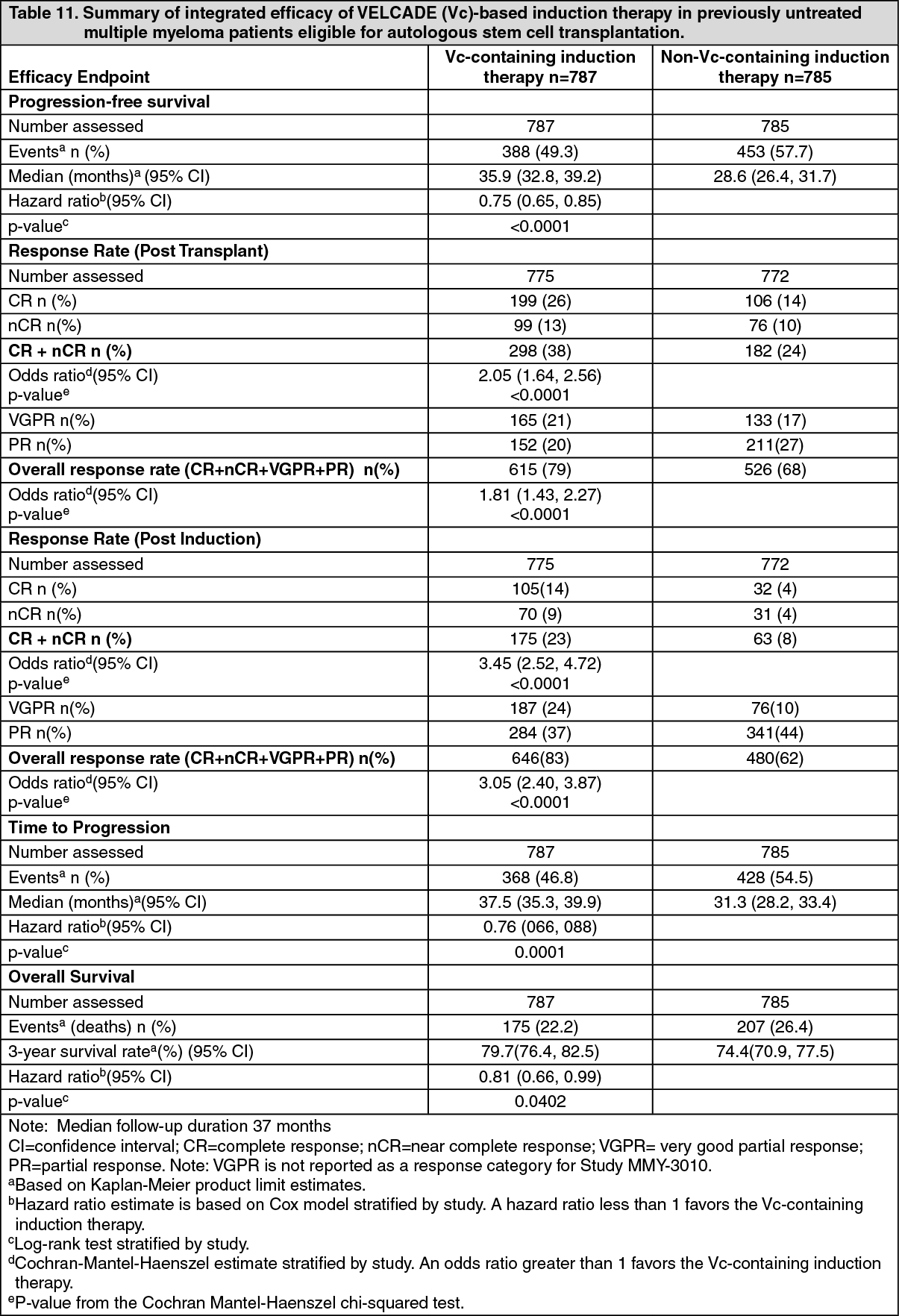
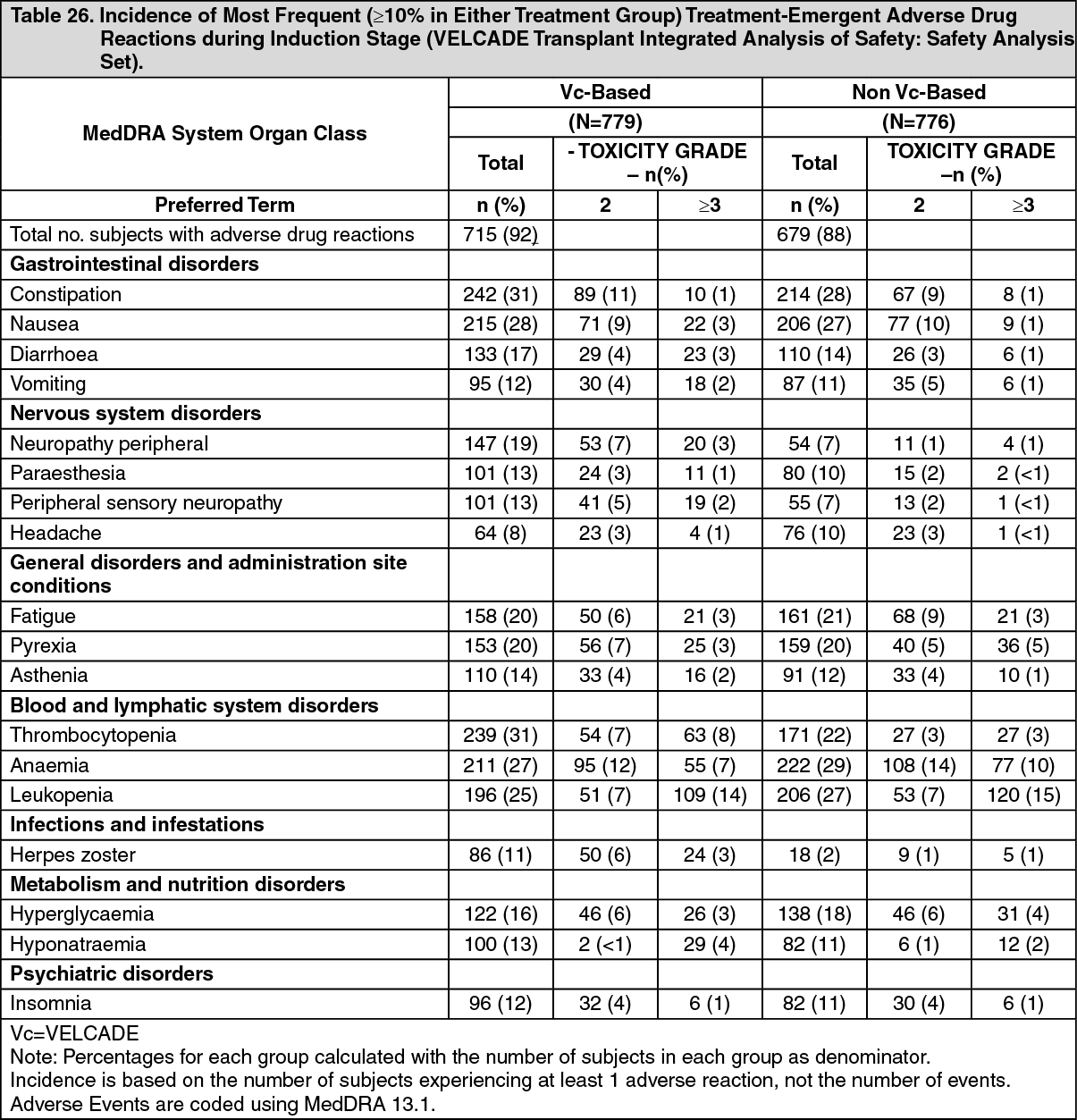
Previously Untreated Multiple Myeloma Patients Eligible for Autologous Stem Cell Transplantation: An integrated data analysis was conducted of three phase 3 trials (MMY-3003, IFM-2005-01, MMY-3010) to demonstrate the safety and efficacy of VELCADE, as induction therapy prior to stem cell transplantation in patients with previously untreated multiple myeloma. These studies were similar in design (randomized, open-label, multicenter) and included 1572 patients (men and women up to 65 years of age with previously untreated multiple myeloma [Durie-Salmon stage II or III] and ECOG PS of 0 to 2/3). Patients received either a VELCADE-containing induction regimen (n=787) or a non-VELCADE-containing induction regimen (n=785). These studies evaluated VELCADE in combination with: 1) dexamethasone and adriamycin (MMY-3003), 2) thalidomide and dexamethasone (MMY-3010), or 3) dexamethasone alone (IFM-2005-01). VELCADE-containing induction regimens were compared to regimens including vincristine, adriamycin and dexamethasone or thalidomide and dexamethasone.
The VELCADE-based treatment group had improved PFS and TTP compared with the non-VELCADE-based treatment group. In addition, patients who received a VELCADE-containing induction regimen had improved post transplant and post induction response rates compared to those who received a non-VELCADE-containing induction regimen.
Integrated efficacy results from studies MMY-3003, IFM-2005-01, MMY-3010 are summarized in the following table: See table 11.
Click on icon to see table/diagram/image
A fourth phase 3 randomized, open-label, multicenter trial (MMY-3006) was conducted in 480 patients (men and women aged 18 to 65 years of age with previously untreated multiple myeloma).
4 In this study, VELCADE-containing induction regimens were compared to regimens containing thalidomide and dexamethasone. The results of this study were consistent with those of the integrated analysis demonstrating improved post–induction CR+nCR rates (31% versus 11% ; p<0.0001), post-transplant CR+nCR rates (55% versus 41%; p=0.0025), and a 37% reduction in the risk of disease progression or death (HR = 0.63 [95% CI: 0.45, 0.88]; p=0.0061) with the VELCADE-based induction regimen as compared with its non-VELCADE-based comparator regimen. The safety profile in the VELCADE-containing regimen was consistent with the known safety profile of VELCADE.
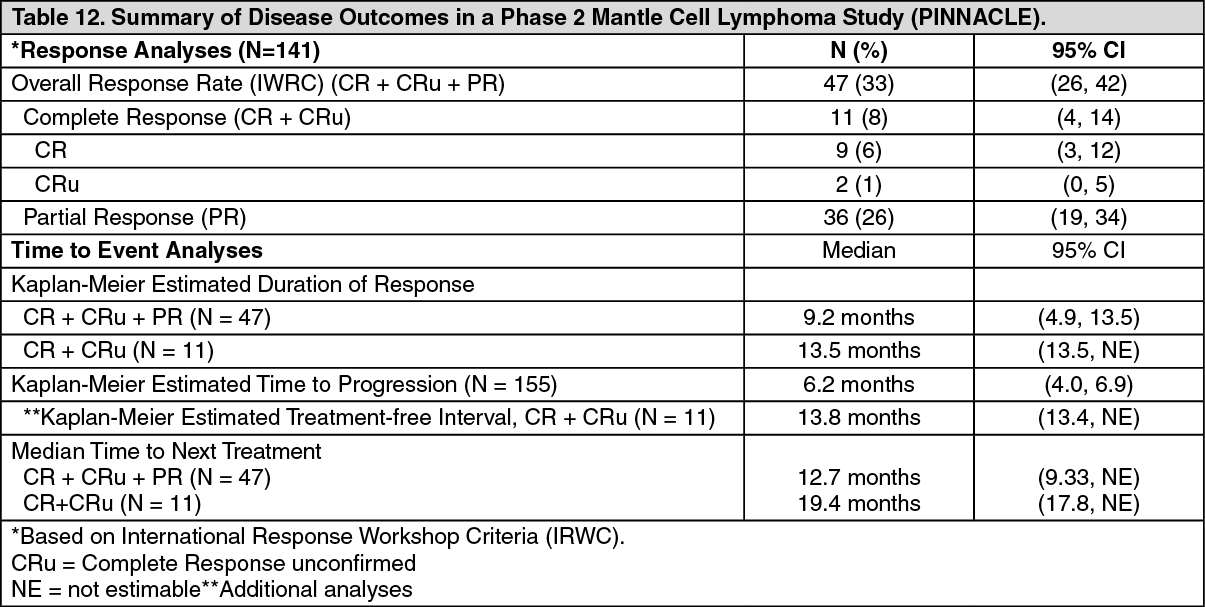
A Phase 2 Single-arm Clinical Study in Relapsed Mantle Cell Lymphoma After Prior therapy: The safety and efficacy of VELCADE in relapsed or refractory mantle cell lymphoma were evaluated in an open-label, single-arm, multicenter study [M34103-053 (PINNACLE)] of 155 patients with progressive disease who had received at least 1 prior therapy. VELCADE was administered at the recommended dose of 1.3 mg/m
2. The median number of cycles administered across all patients was 4 (range 1-17); and 8 in responding patients. Response rates to VELCADE are described in Table 12.
Click on icon to see table/diagram/image
With a median duration of follow up of more than 13 months in surviving patients, the median survival had not yet been reached and the Kaplan Meier estimate of 1-year survival was 69%. The Kaplan-Meier estimate of 1-year survival was 94% in responders and 100% in those achieving CR or CRu.
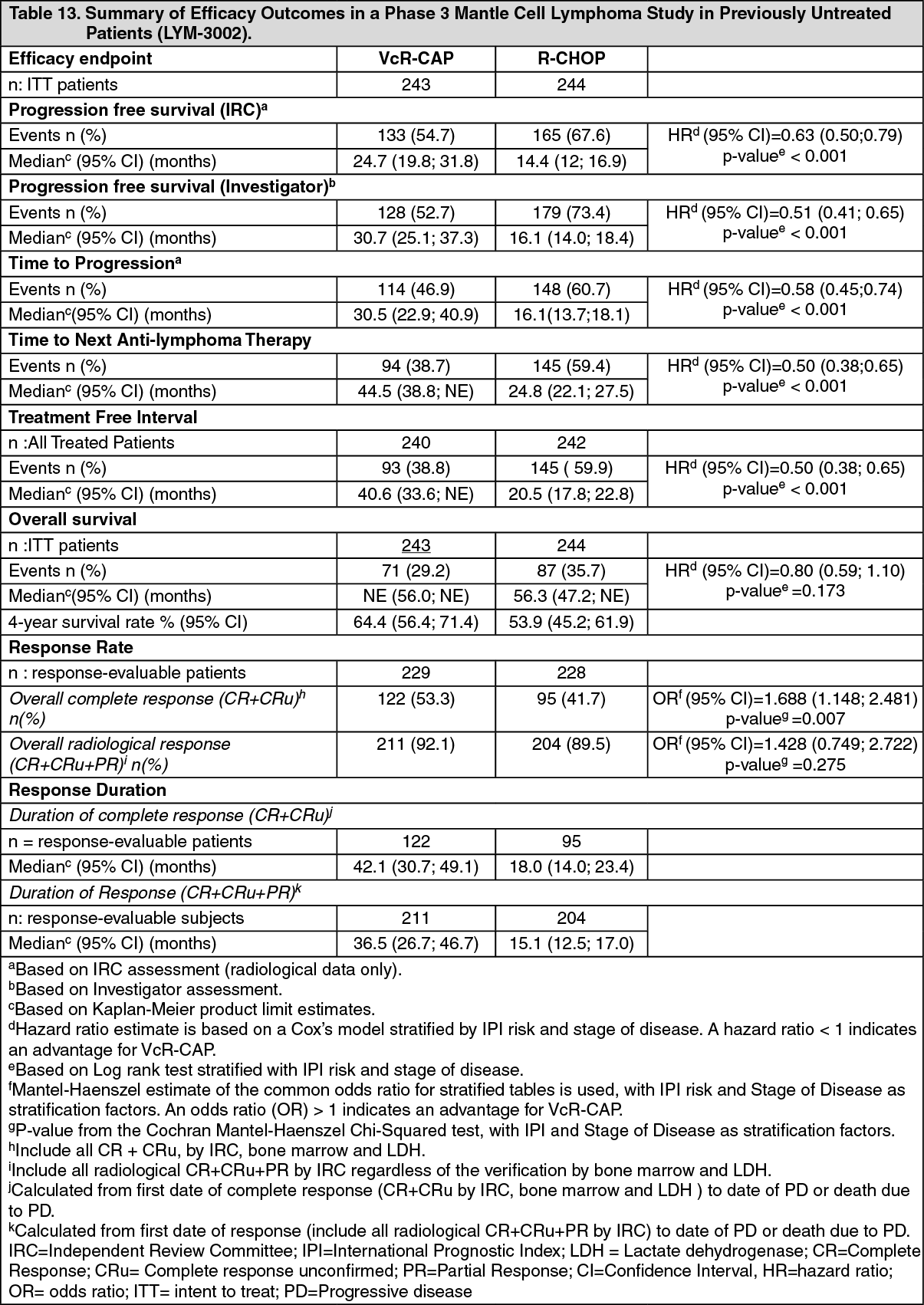
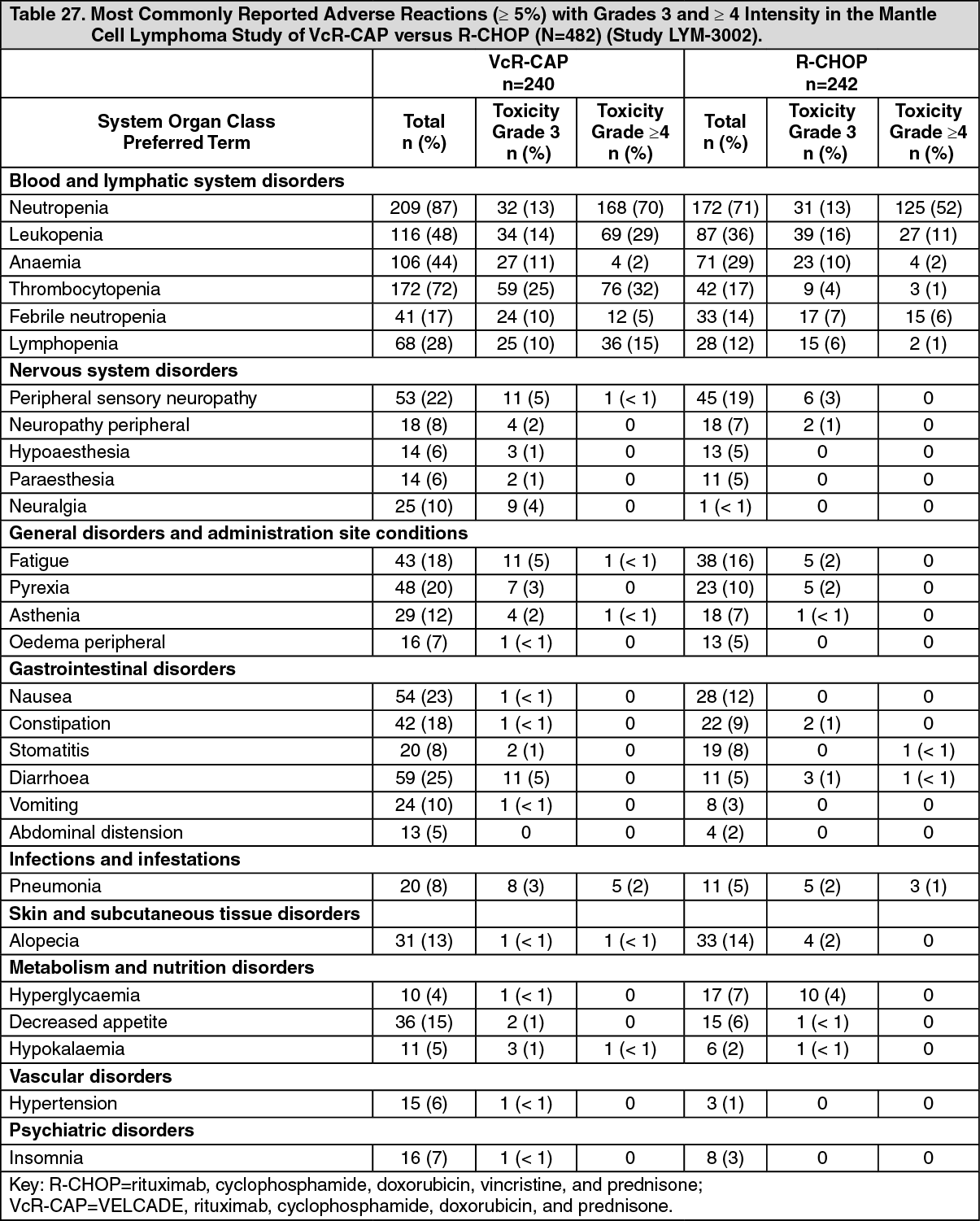
Previously Untreated Mantle Cell Lymphoma: A randomized, open-label, Phase 3 study (LYM-3002) was conducted in 487 adult patients with previously untreated mantle cell lymphoma (Stage II, III or IV) to determine whether VELCADE administered in combination with rituximab, cyclophosphamide, doxorubicin, and prednisone (VcR-CAP) resulted in improvement in progression free survival (PFS) when compared to the combination of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP). This clinical study utilized independent pathology confirmation and independent radiologic response assessment.
Patients in the VcR-CAP treatment arm received VELCADE (1.3 mg/m
2) administered intravenously on Days 1, 4, 8, and 11 (rest period Days 12-21); rituximab (375 mg/m
2) on Day 1; cyclophosphamide (750 mg/m
2) on Day 1; doxorubicin (50 mg/m2) on Day 1; and prednisone (100 mg/m
2) on Day 1 through Day 5 of the 21-day treatment cycle. For patients with a response first documented at Cycle 6, two additional treatment cycles were given.
Median patient age was 66 years, 74% were male, 66% were Caucasian and 32% were Asian. 69% of patients had a positive bone marrow aspirate and/or a positive bone marrow biopsy for MCL, 35% of patients had an International Prognostic Index (IPI) score of 3 (high-intermediate) and 74% had Stage IV disease. Median number of cycles received by patients in both treatment arms was 6 with 17% of patients in the R-CHOP group and 14% of subjects in the VcR-CAP group receiving up to 2 additional cycles. The majority of the patients in both groups received 6 or more cycles of treatment, 83% in the R-CHOP group and 84% in the VcR-CAP group.
The primary efficacy endpoint was progression-free survival based on Independent Review Committee (IRC) assessment. Secondary endpoints included, time to progression (TTP), time to next anti-lymphoma treatment (TNT), duration of treatment free interval (TFI), overall response rate (ORR) and complete response (CR/CRu) rate, overall survival (OS) and response duration. The response criteria used to assess efficacy were based on the International Workshop to Standardize Response Criteria for Non-Hodgkin's Lymphoma (IWRC)
6.
A 59% improvement in the primary endpoint of PFS (Hazard Ratio [HR]=0.63; p<0.001) was observed in the VcR-CAP group (median=24.7 months) as compared to the R-CHOP group (median=14.4 months). A statistically significant benefit in favor of the VcR-CAP treatment group was observed for TTP, TNT, TFI and the overall complete response rate. The median duration of complete response was more than double in the VcR-CAP group (42.1 months) compared with the R-CHOP group (18 months) and the duration of overall response was 21.4 months longer in the VcR-CAP group. With a median duration of follow-up of 40 months, median OS (56.3 months in the R-CHOP group, and not reached in the VcR CAP group) favored the VcR-CAP group, (estimated HR=0.80; p=0.173). There was a trend towards prolonged overall survival favoring the VcR-CAP group; the estimated 4-year survival rate was 53.9% in the R-CHOP group and 64.4% in the VcR-CAP group. Efficacy results at a median follow-up of 40 months are presented in Table 13.
Click on icon to see table/diagram/image
Patients with previously treated light-chain (AL) Amyloidosis: A Phase 1/2 study was conducted to determine the safety and efficacy of VELCADE in patients with previously treated light-chain (AL) Amyloidosis. No new safety concerns were observed during the study, and in particular VELCADE did not exacerbate target organ damage (heart, kidney and liver). In 49 evaluable patients treated at 1.6 mg/m
2 weekly or 1.3 mg/m
2 twice-weekly, a 67.3% response rate (including a 28.6% CR rate) as measured by haematological response (M- protein) was reported. For these dose cohorts, the combined 1 year survival rate was 88.1%.
Pediatric Use: The safety and effectiveness of VELCADE in pediatric patients has not been established.
Geriatric Use: No overall differences in safety or effectiveness were observed between patients ≥age 65 and younger patients receiving VELCADE; in the patients studied with multiple myeloma and mantle cell lymphoma, but greater sensitivity of some older individuals cannot be ruled out.
Pharmacokinetics: Following intravenous bolus administration of a 1.0 mg/m
2 and 1.3 mg/m
2 dose to eleven patients with multiple myeloma, the mean first-dose maximum plasma concentrations of bortezomib were 57 and 112 ng/ml respectively. In subsequent doses, mean maximum observed plasma concentrations ranged from 67 to 106 ng/ml for the 1.0 mg/m
2 dose and 89 to 120 ng/ml for the 1.3 mg/m
2 dose. The mean elimination half-life of bortezomib upon multiple dosing ranged from 40-193 hours. Bortezomib is eliminated more rapidly following the first dose compared to subsequent doses. Mean total body clearances were 102 and 112 l/h following the first dose for doses of 1.0 mg/m
2 and 1.3 mg/m
2, respectively, and ranged from 15 to 32 l/h following subsequent doses for doses of 1.0 mg/m
2 and 1.3 mg/m
2, respectively.
In the PK/PD substudy in Phase 3 trial, following an IV bolus or subcutaneous (SC) injection of a 1.3 mg/m
2 dose to multiple myeloma patients (n=14 for IV, n=17 for SC), the total systemic exposure after repeat dose administration (AUC
last) was equivalent for SC and IV administration. The C
max after SC administration (20.4 ng/mL) was lower than IV (223 ng/mL). The AUC
last geometric mean ratio was 0.99 and 90% confidence intervals were 80.18%-122.80%.
Distribution: The mean distribution volume of bortezomib ranged from 1659 liters to 3294 liters (489 to 1884 l/m
2) single- or repeat-dose IV administration of 1.0 mg/m
2 or 1.3 mg/m
2 to patients with multiple myeloma. This suggests that bortezomib distributes widely to peripheral tissues. The binding of bortezomib to human plasma proteins averaged 83% over the concentration range of 100-1000 ng/ml.
Metabolism: In vitro studies with human liver microsomes and human cDNA-expressed cytochrome P450 isozymes indicate that bortezomib is primarily oxidatively metabolized via cytochrome P450 enzymes, 3A4, 2C19, and 1A2. Bortezomib metabolism by CYP 2D6 and 2C9 enzymes is minor. The major metabolic pathway is deboronation to form two deboronated metabolites that subsequently undergo hydroxylation to several metabolites. Deboronated-bortezomib metabolites are inactive as 26S proteasome inhibitors. Pooled plasma data from 8 patients at 10 min and 30 min after IV dosing indicate that the plasma levels of metabolites are low compared to the parent drug.
Elimination: The pathways of elimination of bortezomib have not been characterized in humans.
Special Populations: Age, Gender, and Race:
The pharmacokinetics of bortezomib were characterized following twice weekly intravenous bolus administration of 1.3 mg/m
2 doses to 104 pediatric patients (2-16 years old) with acute lymphoblastic leukemia (ALL) or acute myeloid leukemia (AML). Based on a population pharmacokinetic analysis, clearance of bortezomib increased with increasing body surface area (BSA). Geometric mean (%CV) clearance was 7.79 (25%) L/hr/m
2, volume of distribution at steady-state was 834 (39%) L/m
2, and the elimination half-life was 100 (44%) hours. After correcting for the BSA effect, other demographics such as age, body weight and sex did not have clinically significant effects on bortezomib clearance. BSA-normalized clearance of bortezomib in pediatric patients was similar to that observed in adults.
The effects of gender and race on the pharmacokinetics of bortezomib have not been evaluated.
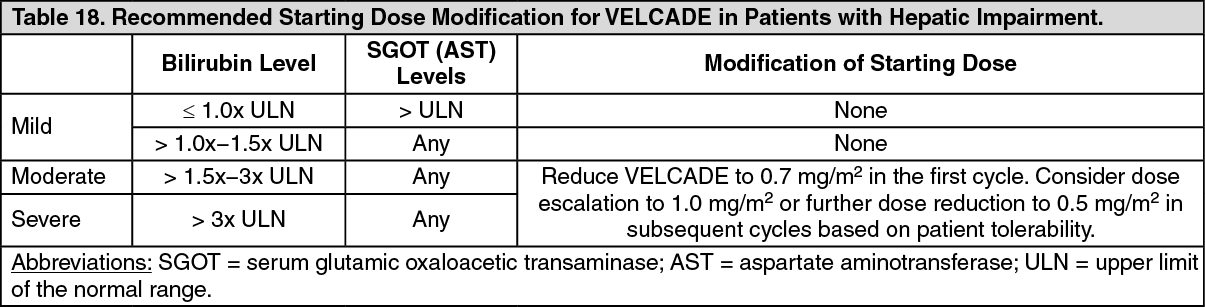
Hepatic Impairment: The effect of hepatic impairment on the pharmacokinetics of IV bortezomib was assessed in 60 cancer patients at bortezomib doses ranging from 0.5 to 1.3 mg/m
2. When compared to patients with normal hepatic function, mild hepatic impairment did not alter dose-normalized bortezomib AUC. However, the dose-normalized mean AUC values were increased by approximately 60% in patients with moderate or severe hepatic impairment. A lower starting dose is recommended in patients with moderate or severe hepatic impairment, and those patients should be monitored closely (see Table 18).
Renal Impairment:
A pharmacokinetic study was conducted in patients with various degrees of renal impairment who were classified according to their creatinine clearance values (CrCL) into the following groups: Normal (CrCL ≥60 ml/min/1.73 m
2, n=12), Mild (CrCL= 40-59 ml/min/1.73 m
2, n=10), Moderate (CrCL=20-39 ml/min/1.73 m
2, n=9), and Severe (CrCL <20 ml/min/1.73 m
2, n=3). A group of dialysis patients who were dosed after dialysis was also included in the study (n=8). Patients were administered intravenous doses of 0.7 to 1.3 mg/m
2 of bortezomib twice weekly. Exposure of bortezomib (dose-normalized AUC and C
max) was comparable among all the groups (see Dosage & Administration).
Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenicity studies have not been conducted with bortezomib.
Bortezomib showed clastogenic activity (structural chromosomal aberrations) in the
in vitro chromosomal aberration assay using Chinese hamster ovary cells. Bortezomib was not genotoxic when tested in the
in vitro mutagenicity assay (Ames test) and
in vivo micronucleus assay in mice.
Fertility studies with bortezomib were not performed but evaluation of reproductive tissues has been performed in the general toxicity studies. In the 6-month rat toxicity study, degenerative effects in the ovary were observed at doses ≥0.3 mg/m
2 (one-fourth of the recommended clinical dose), and degenerative changes in the testes occurred at 1.2 mg/m
2. VELCADE could have a potential effect on either male or female fertility.



 Sign Out
Sign Out