


 Sign Out
Sign Out

 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image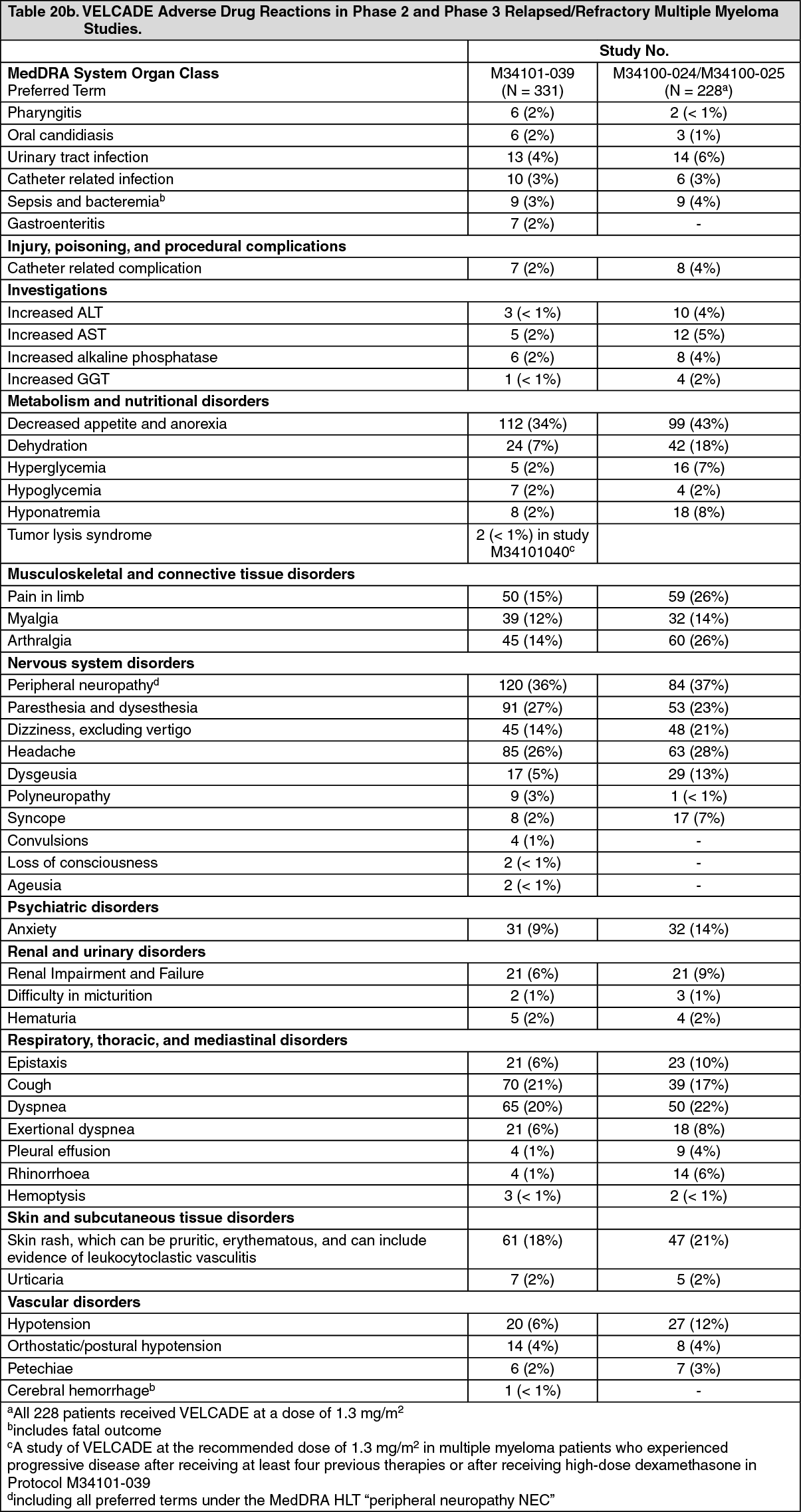 Click on icon to see table/diagram/image
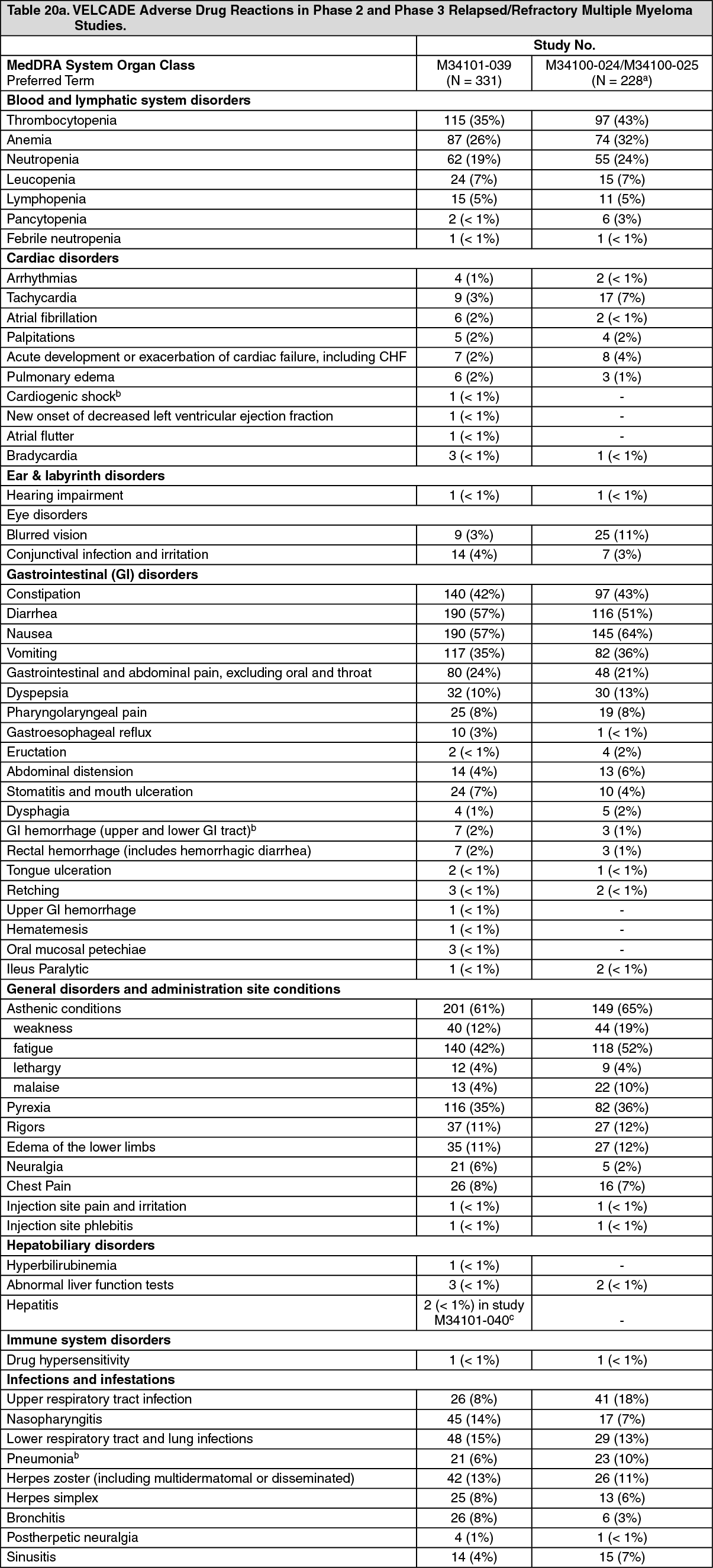
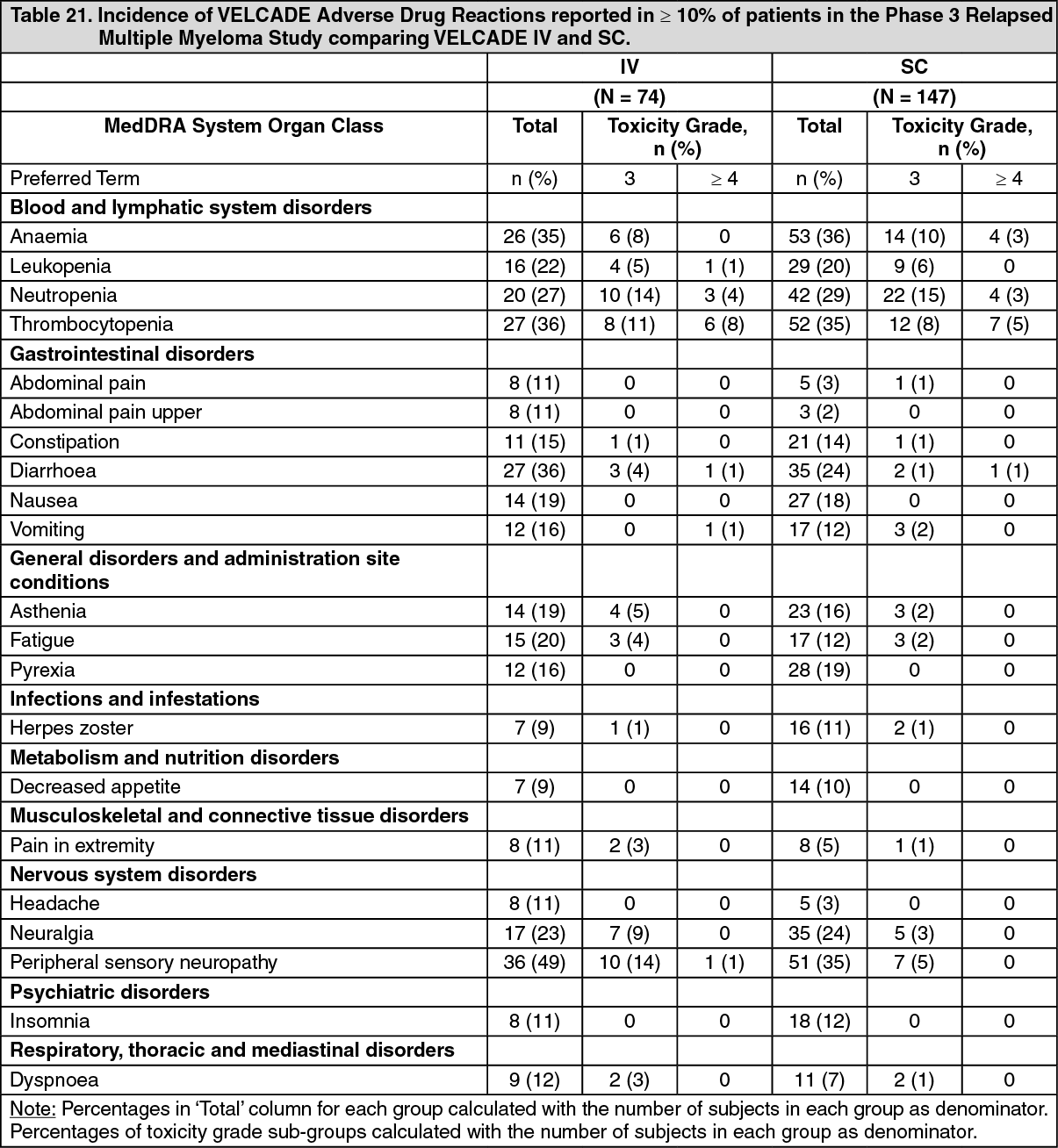
Click on icon to see table/diagram/imageSummary of Clinical Trials of VELCADE IV vs SC in Patients with Relapsed Multiple Myeloma: The safety and efficacy of VELCADE SC were evaluated in one Phase 3 study at the recommended dose of 1.3 mg/m2. This was a randomized, comparative study of VELCADE IV vs SC in 222 patients with relapsed multiple myeloma. (See Table 21.)
 Click on icon to see table/diagram/image
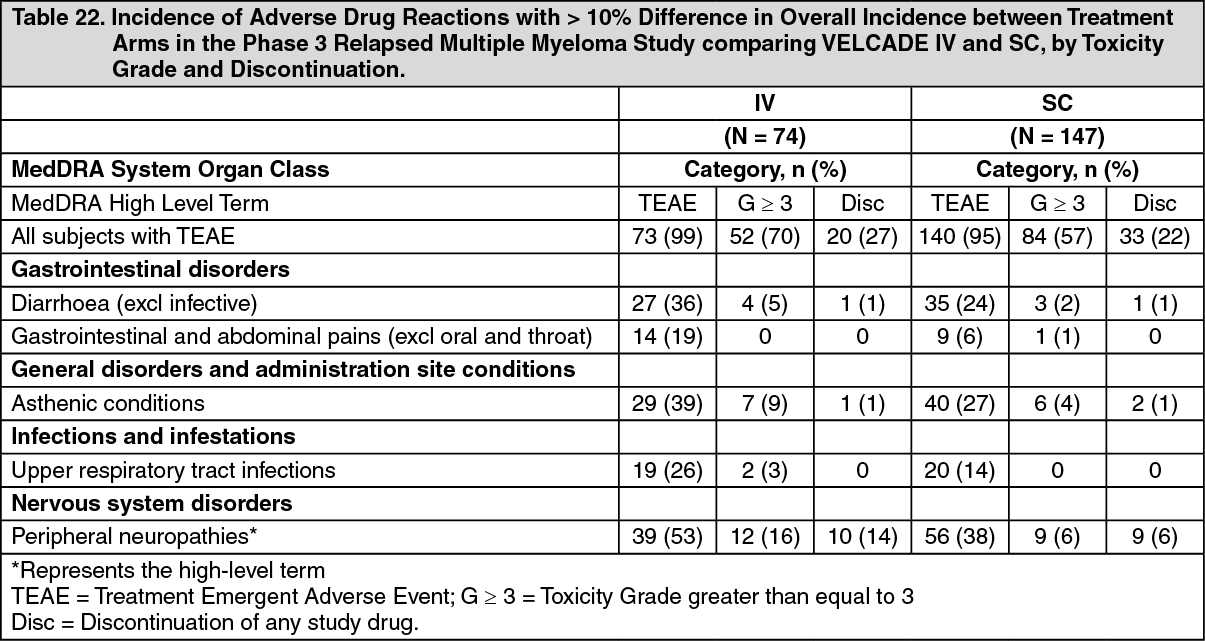
Click on icon to see table/diagram/imageAlthough, in general safety data were similar for the IV and SC treatment groups, the following table highlights differences larger than 10% in the overall incidence of adverse drug reactions between the two treatment arms. (See Table 22.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients who received VELCADE subcutaneously compared to intravenous administration had 13% lower overall incidence of treatment emergent adverse drug reactions that were grade 3 or higher in toxicity (57% vs 70% respectively), and a 5% lower incidence of discontinuation of VELCADE (22% vs 27%). The overall incidence of diarrhea (24% for the SC arm vs 36% for the IV arm), gastrointestinal and abdominal pain (6% for the SC arm vs 19% for the IV arm), asthenic conditions (27% for SC arm vs 39% for IV arm), upper respiratory tract infections (14% SC arm vs 26% IV arm) and peripheral neuropathy NEC (38% SC arm vs 53% IV arm) were 12%-15% lower in the subcutaneous group than the intravenous group. In addition, the incidence of peripheral neuropathies that were grade 3 or higher in toxicity was 10% lower (6% for SC vs 16% for IV), and the discontinuation rate due to peripheral neuropathies was 8% lower for the subcutaneous group (5%) as compared to the intravenous group (12%).
Six percent of patients were reported to have had an adverse local reaction to SC administration, mostly redness. Only 2 (1%) subjects were reported as having severe reactions. These severe local reactions were 1 case of pruritus and 1 case of redness. These reactions seldom led to dose modifications and all resolved in a median of 6 days.
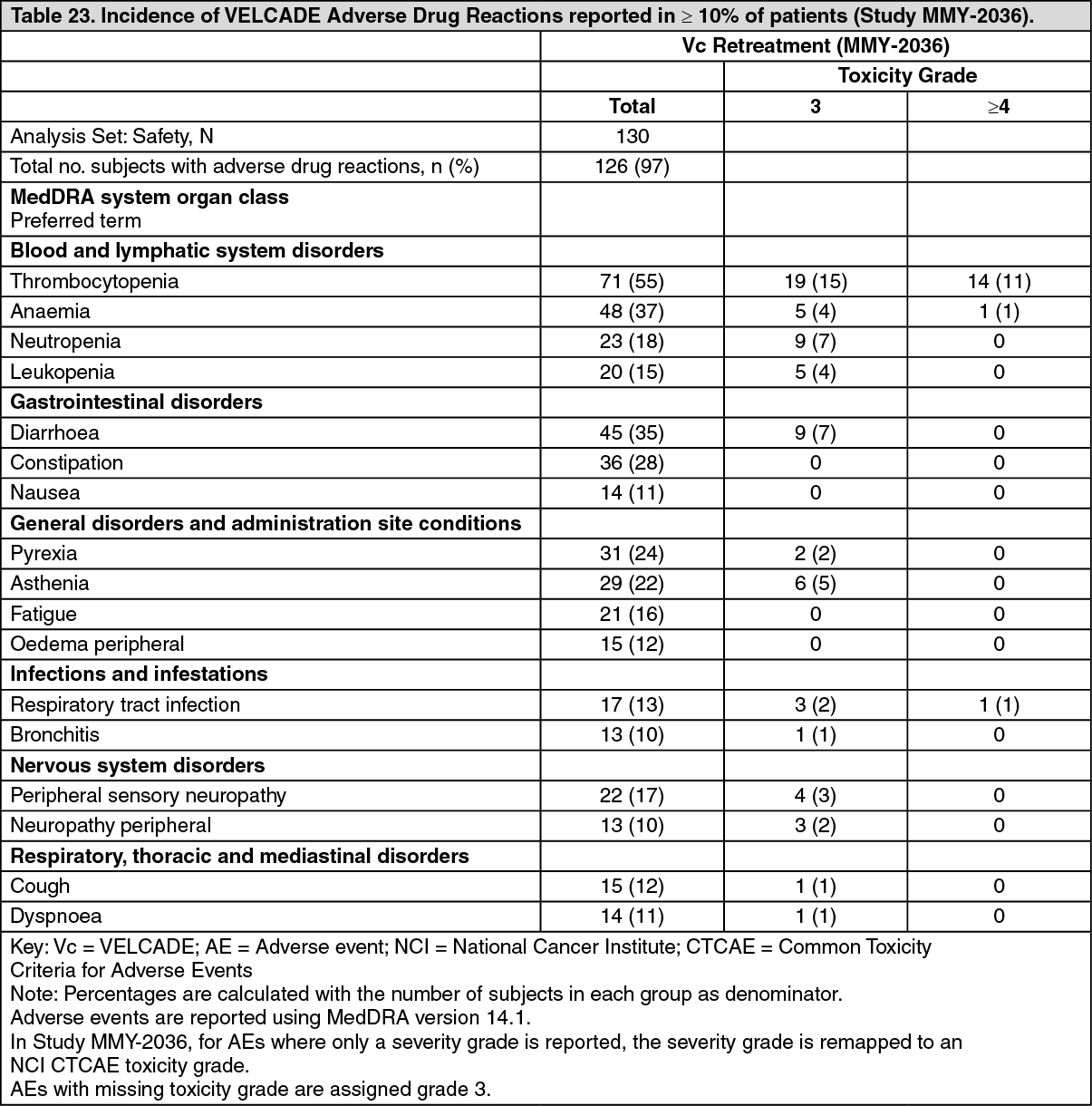
VELCADE Retreatment in Relapsed Multiple Myeloma: The following table describes adverse drug reactions reported for at least 10% of patients with relapsed multiple myeloma who received retreatment with VELCADE IV (Study MMY-2036). (See Table 23.)
 Click on icon to see table/diagram/image
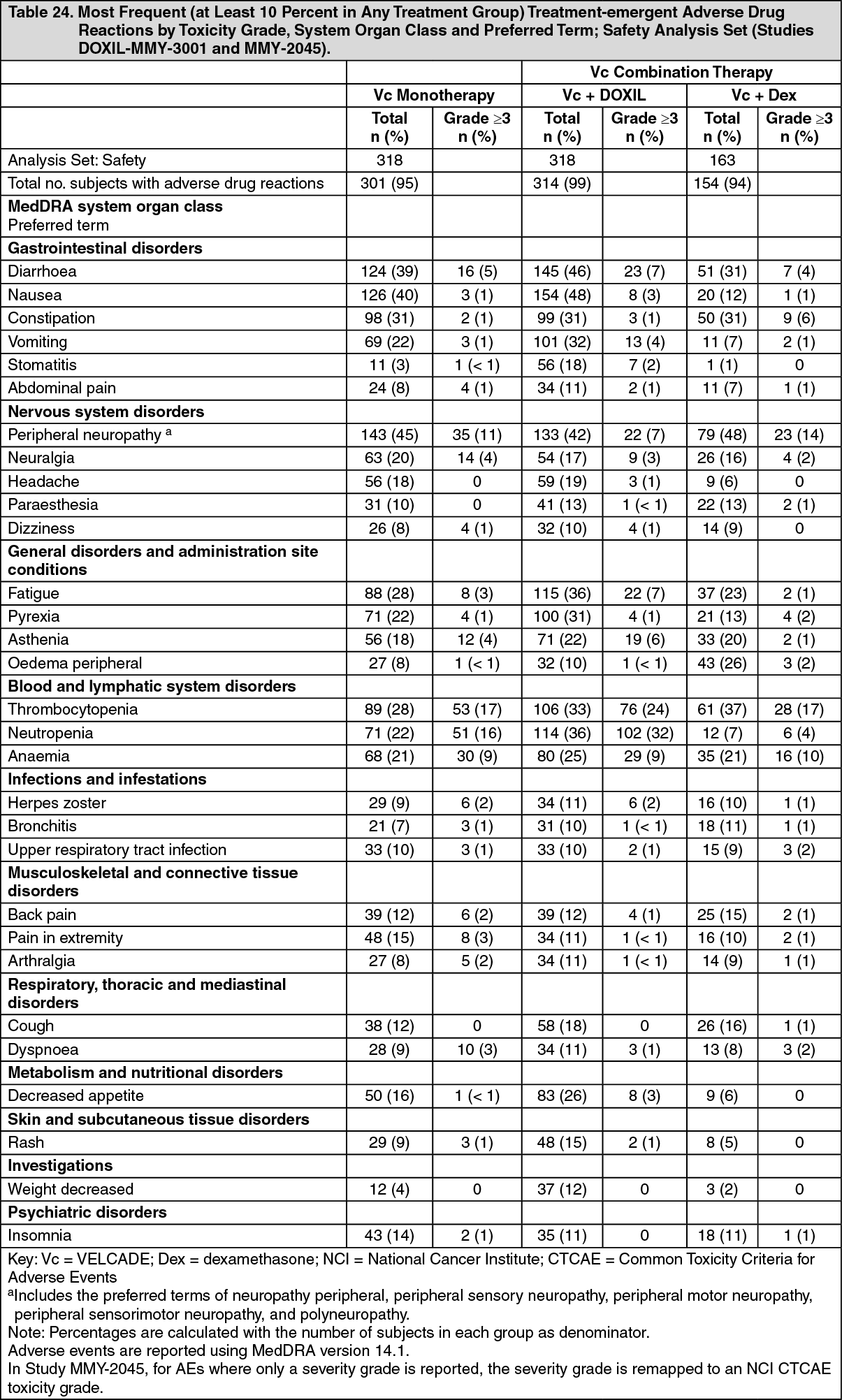
Click on icon to see table/diagram/imageSummary of Clinical Trials of VELCADE Combination Therapy in Patients with Relapsed Multiple Myeloma: The following table describe adverse drug reactions reported for at least 10% of patients with relapsed multiple myeloma who received VELCADE in combination with dexamethasone (Study MMY-2045) or VELCADE in combination with pegylated liposomal doxorubicin (Study DOXIL-MMY-3001). (See Table 24.)
 Click on icon to see table/diagram/image
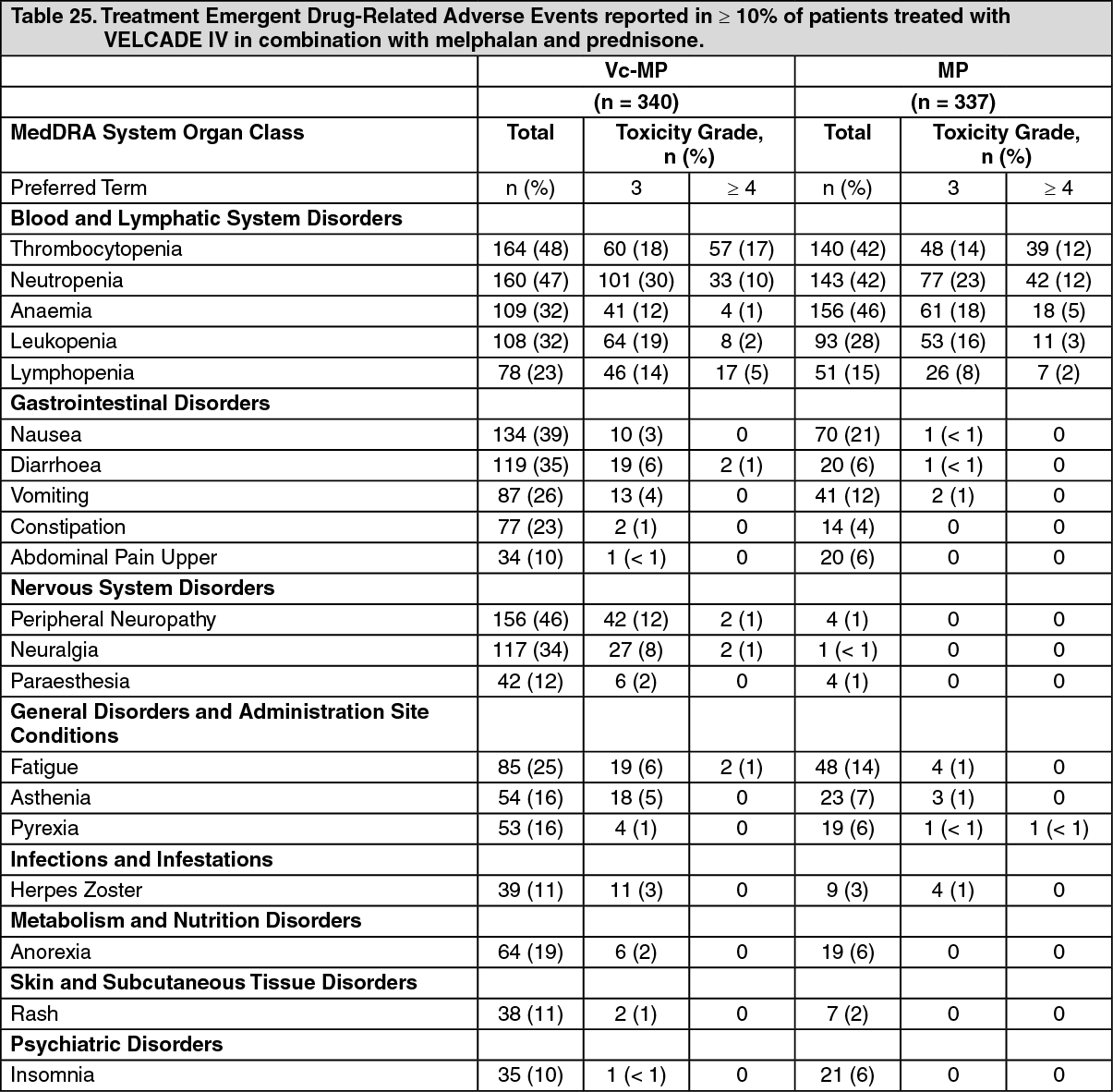
Click on icon to see table/diagram/imageSummary of Clinical Trials in patients with previously untreated multiple myeloma: The following table describes safety data from 340 patients with previously untreated multiple myeloma who received VELCADE IV (1.3 mg/m2) in combination with melphalan (9 mg/m2) and prednisone (60 mg/m2) in a prospective phase 3 study. (See Table 25.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHerpes zoster virus reactivation: Physicians should consider using antiviral prophylaxis in patients being treated with VELCADE. In the phase 3 study in patients with previously untreated multiple myeloma, the overall incidence of herpes zoster reactivation was more common in patients treated with VcMP compared with MP (14% vs 4% respectively). Antiviral prophylaxis was administered to 26% of the patients in the VcMP arm. The incidence of herpes zoster among patients in the VcMP treatment group was 17% for patients not administered antiviral prophylaxis compared to 3% for patients administered antiviral prophylaxis.
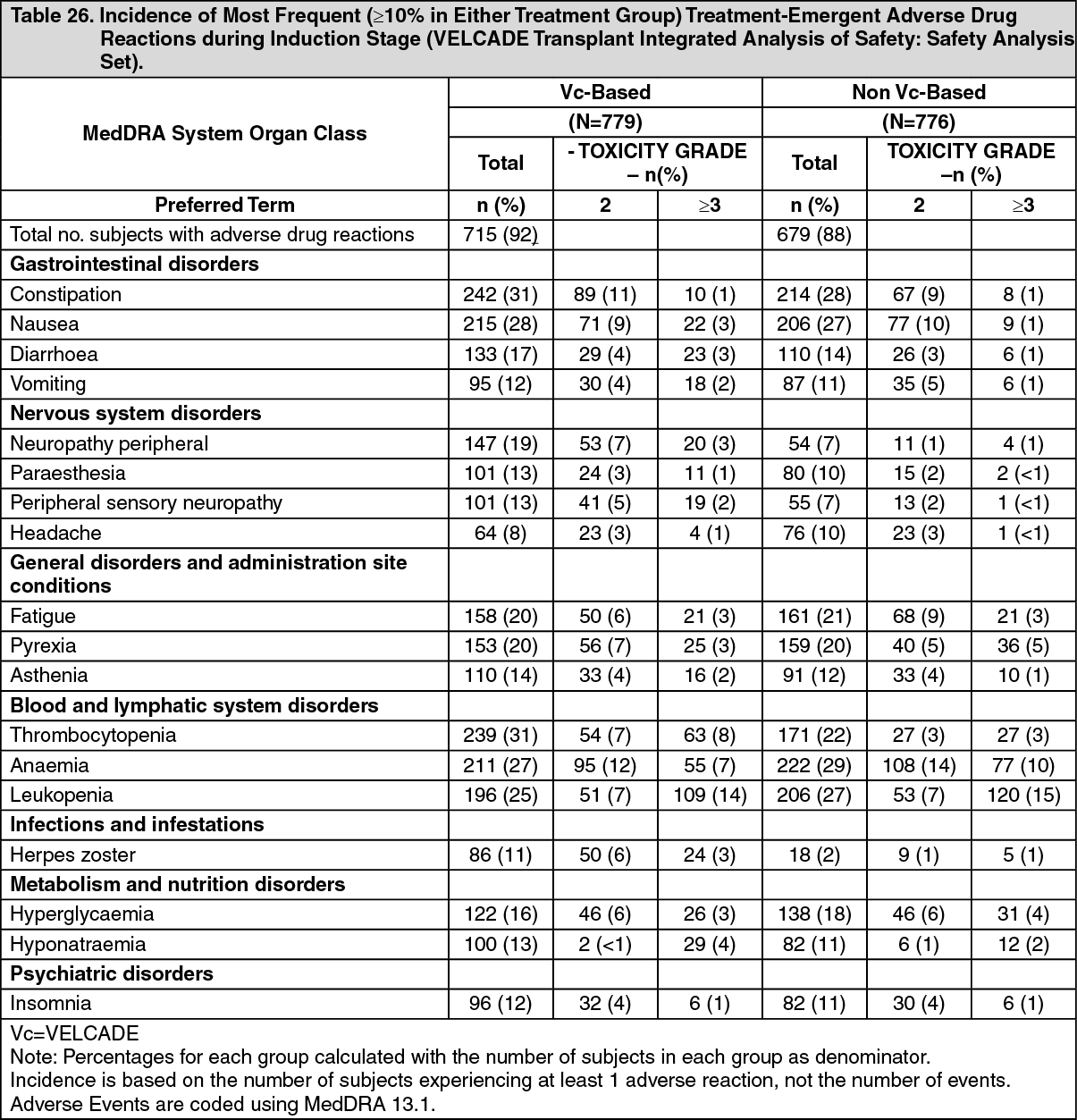
The following table describes adverse drug reactions considered by the Company to have at least a possible causal relationship to VELCADE from patients with previously untreated multiple myeloma eligible for stem cell transplantation who received VELCADE IV (1.3 mg/m2). 410 patients were treated with VELCADE in combination with doxorubicin and dexamethasone compared with 411 patients treated with vincristine, doxorubicin and dexamethasone in Study MMY-3003, 239 were treated with VELCADE in combination with dexamethasone alone compared with 239 patients treated with vincristine, doxorubicin and dexamethasone in Study IFM 2005-01, and 130 were treated with VELCADE in combination with thalidomide and dexamethasone compared with 126 patients treated with thalidomide and dexamethasone in Study MMY-3010. For these 3 studies conducted in the transplant setting (MMY3003, IFM2005-01, MMY3010), only the adverse reactions during the induction phase of treatment are considered for the table. (See Table 26.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSummary of the Clinical Trial in Patients with Relapsed Mantle Cell Lymphoma: Safety data for patients with relapsed mantle cell lymphoma were evaluated in a phase 2 study [M34103-053 (PINNACLE)], which included 155 patients treated with VELCADE at the recommended dose of 1.3 mg/m2. The safety profile of VELCADE in these patients was similar to that observed in patients with multiple myeloma. Notable differences between the two patient populations were that thrombocytopenia, neutropenia, anemia, nausea, vomiting and pyrexia were reported more often in the patients with multiple myeloma than in those with mantle cell lymphoma; whereas peripheral neuropathy, rash and pruritis were higher among patients with mantle cell lymphoma compared to patients with multiple myeloma.
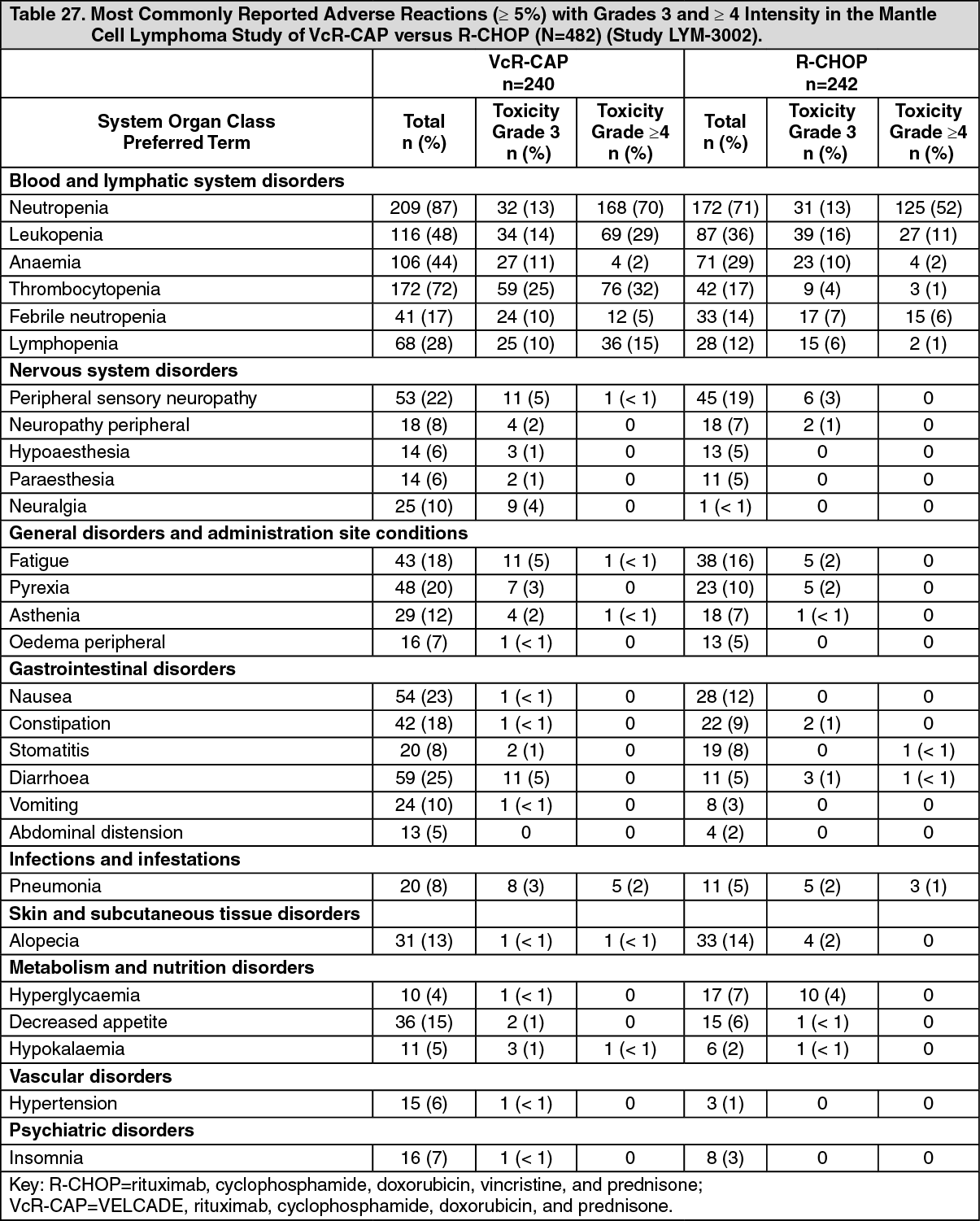
Summary of Clinical Trial in Patients with Previously Untreated Mantle Cell Lymphoma: Table 27 describes safety data from 240 patients with previously untreated mantle cell lymphoma who received VELCADE (1.3 mg/m2) administered IV in combination with rituximab (375 mg/m2), cyclophosphamide (750 mg/m2), doxorubicin (50 mg/m2), and prednisone (100 mg/m2) (VcR-CAP) in a prospective randomized study.
The incidences of Grade ≥3 bleeding events were similar between the 2 arms (3 patients in the VcR-CAP arm and 1 patient in the R-CHOP arm). All of the Grade ≥3 bleeding events resolved without sequelae in the VcR-CAP arm.
Infections were reported for 31% of patients in the VcR-CAP arm and 23% of the patients in the R-CHOP arm. Respiratory tract and lung infections were reported, with the predominant preferred term of pneumonia (VcR-CAP 8% versus R CHOP 5%).
The incidence of herpes zoster reactivation was 4.6% in the VcR-CAP arm and 0. 8% in the R-CHOP arm. Antiviral prophylaxis was mandated by protocol amendment. (See Table 27.)
 Click on icon to see table/diagram/image
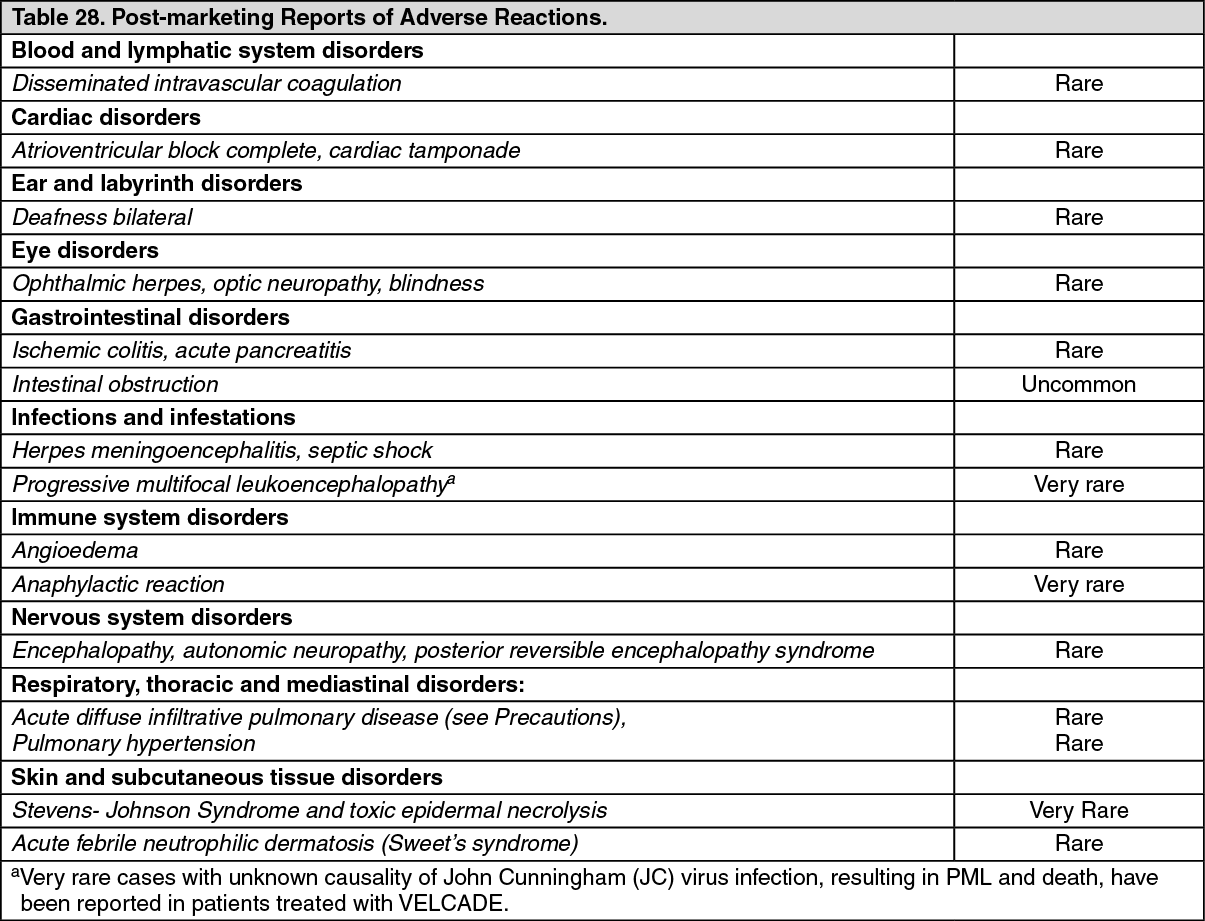
Click on icon to see table/diagram/imagePost-Marketing Experience: Clinically significant adverse drug reactions are listed here if they have not been reported previously.
The frequencies provided as follows reflect reporting rates of adverse drug reactions from the worldwide post-marketing experience with VELCADE. The frequencies provided as follows reflect reporting rates and precise estimates of incidence cannot be made. These adverse drug reactions are ranked by frequency, using the following convention: Very common (≥1/10), common (≥1/100 and <1/10), uncommon (≥1/1000 and <1/100), rare (≥1/10,000 and <1/1000), very rare (<1/10,000 including isolated reports). (See Table 28.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form