


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Topiramate is classified as a sulfamate-substituted monosaccharide. The precise mechanism by which topiramate exerts its antiseizure and migraine prophylaxis effects are unknown. Electrophysiological and biochemical studies on cultured neurons have identified three properties that may contribute to the antiepileptic efficacy of topiramate.
Action potentials elicited repetitively by a sustained depolarization of the neurons were blocked by topiramate in a time-dependent manner, suggestive of a state-dependent sodium channel blocking action. Topiramate increased the frequency at which γ-aminobutyrate (GABA) activated GABAA receptors, and enhanced the ability of GABA to induce a flux of chloride ions into neurons, suggesting that topiramate potentiates the activity of this inhibitory neurotransmitter.
This effect was not blocked by flumazenil, a benzodiazepine antagonist, nor did topiramate increase the duration of the channel open time, differentiating topiramate from barbiturates that modulate GABAA receptors.
Because the antiepileptic profile of topiramate differs markedly from that of the benzodiazepines, it may modulate a benzodiazepine-insensitive subtype of GABAA receptor. Topiramate antagonized the ability of kainate to activate the kainate/AMPA (α-amino-3-hydroxy-5-methylisoxazole-4-propionic acid) subtype of excitatory amino acid (glutamate) receptor, but had no apparent effect on the activity of N-methyl-D-aspartate (NMDA) at the NMDA receptor subtype. These effects of topiramate were concentration-dependent over a range of 1 mcM to 200 mcM, with minimum activity observed at 1 mcM to 10 mcM.
In addition, topiramate inhibits some isoenzymes of carbonic anhydrase. This pharmacologic effect is much weaker than that of acetazolamide, a known carbonic anhydrase inhibitor, and is not thought to be a major component of topiramate’s antiepileptic activity.
In animal studies, topiramate exhibits anticonvulsant activity in rat and mouse maximal electroshock seizure (MES) tests and is effective in rodent models of epilepsy, which include tonic and absence-like seizures in the spontaneous epileptic rat (SER) and tonic and clonic seizures induced in rats by kindling of the amygdala or by global ischemia. Topiramate is only weakly effective in blocking clonic seizures induced by the GABAA receptor antagonist, pentylenetetrazole.
Studies in mice receiving concomitant administration of topiramate and carbamazepine or phenobarbital showed synergistic anticonvulsant activity, while combination with phenytoin showed additive anticonvulsant activity. In well-controlled add-on trials, no correlation has been demonstrated between trough plasma concentrations of topiramate and its clinical efficacy. No evidence of tolerance has been demonstrated in man.
Epilepsy Clinical Trials: The results of controlled clinical trials established the efficacy of TOPAMAX Tablets as monotherapy for adults and children (ages 6 and older) with epilepsy, adjunctive therapy in adults and pediatric patients ages 2-16 years with partial onset seizures or primary generalized tonic-clonic seizures, and in patients 2 years of age and older with seizures associated with Lennox-Gastaut syndrome.
Monotherapy: The effectiveness of topiramate as monotherapy in adults and children 6 years of age and older with newly diagnosed epilepsy was established in 4 randomized, double-blind, parallel-group trials. Study EPMN-106 was conducted in 487 patients (6 to 83 years of age) who had a new diagnosis of epilepsy (partial onset or generalized) or a diagnosis of recurrent epilepsy while not taking AEDs. Patients were randomized to receive topiramate 50 mg/day or topiramate 400 mg/day. Patients remained in the double-blind phase until they experienced a first partial onset or generalized tonic-clonic seizure, until termination of the double-blind phase 6 months after randomization of the last subject, or until withdrawal for protocol-specified reasons. The primary efficacy assessment was based on the comparison between topiramate dose groups with respect to time to first partial onset or generalized tonic-clonic seizure during the double-blind phase. Comparison of the Kaplan-Meier survival curves of time to first seizure favored topiramate 400 mg/day over topiramate 50 mg/day (p=0.0002, log rank test). The separation between the groups in favor of the higher dose group occurred early in the titration phase and was statistically significant as early as 2 weeks post randomization (p=0.046), when, by following the weekly titration schedule, the subjects in the higher dose group had achieved a maximum topiramate dose of 100 mg/day. The higher dose group was also superior to the lower dose group with respect to the proportion of subjects who remained seizure-free, based on the Kaplan-Meier estimates, for a minimum of 6 months of therapy (82.9% vs. 71.4%; p=0.005), and for a minimum of 1 year of therapy (75.7% vs. 58.8%; p=0.001). The ratio of hazard rates for time to first seizure was 0.516 (95% confidence interval, 0.364 to 0.733). The treatment effects with respect to time to first seizure were consistent across various subject subgroups defined by age, sex, geographic region, baseline body weight, baseline seizure type, time since diagnosis, and baseline AED use.
In study YI, a single center study, patients ages 15-63 with refractory partial onset seizures (n=48) were converted from their existing treatment to TOPAMAX 100 mg/day or 1000 mg/day as monotherapy. The high dose group was statistically superior to the low dose group for efficacy variables. 54% of high dose patients achieved monotherapy compared with 17% in the low dose group with the difference between the doses being statistically significant (p=0.005). The mean time to exit was significantly greater in the high dose group (p=0.002). The investigator and subject global evaluations of clinical response statistically favoured the high dose group (≤0.002).
In study EPMN-104, adult and paediatric patients (ages 6-85) with recently diagnosed epilepsy (n=252) were randomised into the low dose (25 or 50 mg/day) or the high dose group (200 or 500 mg/day) based on their body weight. Overall, 54% of high dose patients and 39% of low dose patients were reported to be seizure free during the double-blind phase (p=0.022). The high dose group was also superior to the low dose group with respect to seizure frequency distribution (p=0.008) and the difference in time to first seizure across three plasma topiramate concentration strata (p=0.015).
In study EPMN-105, patients aged 6-84 with newly diagnosed epilepsy (n=613) were randomised to receive either 100 or 200 mg/day of TOPAMAX or standard anti-epileptic treatment (carbamazepine or valproate). TOPAMAX was at least as efficacious as carbamazepine or valproate in reducing seizures in these patients; the 95% confidence intervals for the difference between the two treatment groups were narrow and included zero, indicating that there were no statistically significant between-group difference. The two treatment groups were also comparable with respect to all clinical utility and efficacy endpoints including time to exit, proportion of seizure-free subjects and time to first seizure.
Patients (n=207; 32 were aged ≤16 years) who completed the double-blind phase of study YI and EPMN-104 were enrolled in long term extension studies with the majority of patients receiving TOPAMAX for 2 to 5 years. In these studies, sustained efficacy was demonstrated with long-term administration of TOPAMAX as monotherapy. There was no significant change in dosage during the extension period and no indication that effectiveness of TOPAMAX monotherapy diminished with continued exposure.
Adjunctive Therapy: Controlled Trials in Patients With Partial Onset Seizures: Adults with Partial Onset Seizures: The effectiveness of topiramate as an adjunctive treatment for adults with partial onset seizures was established in six multicenter, randomized, double-blind, placebo-controlled trials, two comparing several dosages of topiramate and placebo and four comparing a single dosage with placebo, in patients with a history of partial onset seizures, with or without secondarily generalized seizures.
Patients in these studies were permitted a maximum of two AEDs in addition to TOPAMAX Tablets or placebo. In each study, patients were stabilized on optimum dosages of their concomitant AEDs during baseline phase lasting between 4 and 12 weeks. Patients who experienced a prespecified minimum number of partial onset seizures, with or without secondary generalization, during the baseline phase (12 seizures for 12-week baseline, 8 for 8-week baseline, or 3 for 4-week baseline) were randomly assigned to placebo or a specified dose of TOPAMAX Tablets in addition to their other AEDs.
Following randomization, patients began the double-blind phase of treatment. In five of the six studies, patients received active drug beginning at 100 mg per day; the dose was then increased by 100 mg or 200 mg/day increments weekly or every other week until the assigned dose was reached, unless intolerance prevented increases. In the sixth study (119), the 25 or 50 mg/day initial doses of topiramate were followed by respective weekly increments of 25 or 50 mg/day until the target dose of 200 mg/day was reached. After titration, patients entered a 4, 8, or 12-week stabilization period. The numbers of patients randomized to each dose, and the actual mean and median doses in the stabilization period are shown in Tables 2 and 3.
Pediatric Patients Ages 2-16 Years With Partial Onset Seizures: The effectiveness of topiramate as an adjunctive treatment for pediatric patients ages 2-16 years with partial onset seizures was established in a multicenter, randomized, double-blind, placebo-controlled trial, comparing topiramate and placebo in patients with a history of partial onset seizures, with or without secondarily generalized seizures.
Patients in this study were permitted a maximum of two AEDs in addition to TOPAMAX Tablets or placebo. In this study, patients were stabilized on optimum dosages of their concomitant AEDs during an 8-week baseline phase. Patients who experienced at least six partial onset seizures, with or without secondarily generalized seizures, during the baseline phase were randomly assigned to placebo or TOPAMAX Tablets in addition to their other AEDs.
Following randomization, patients began the double-blind phase of treatment. Patients received active drug beginning at 25 or 50 mg per day; the dose was then increased by 25 mg to 150 mg/day increments every other week until the assigned dosage of 125, 175, 225, or 400 mg/day based on patients’ weight to approximate a dosage of 6 mg/kg per day was reached, unless intolerance prevented increases. After titration, patients entered an 8-week stabilization period.
Controlled Trials in Patients With Primary Generalized Tonic-Clonic Seizures: The effectiveness of topiramate as an adjunctive treatment for primary generalized tonic-clonic seizures in patients 2 years old and older was established in a multicenter, randomized, double-blind, placebo-controlled trial, comparing a single dosage of topiramate and placebo.
Patients in this study were permitted a maximum of two AEDs in addition to TOPAMAX or placebo. Patients were stabilized on optimum dosages of their concomitant AEDs during an 8-week baseline phase. Patients who experienced at least three primary generalized tonic-clonic seizures during the baseline phase were randomly assigned to placebo or TOPAMAX in addition to their other AEDs.
Following randomization, patients began the double-blind phase of treatment. Patients received active drug beginning at 50 mg per day for four weeks; the dose was then increased by 50 mg to 150 mg/day increments every other week until the assigned dose of 175, 225, or 400 mg/day based on patients’ body weight to approximate a dosage of 6 mg/kg per day was reached, unless intolerance prevented increases. After titration, patients entered a 12-week stabilization period.
Controlled Trial in Patients With Lennox-Gastaut Syndrome: The effectiveness of topiramate as an adjunctive treatment for seizures associated with Lennox-Gastaut syndrome was established in a multicenter, randomized, double-blind, placebo-controlled trial comparing a single dosage of topiramate with placebo in patients 2 years of age and older.
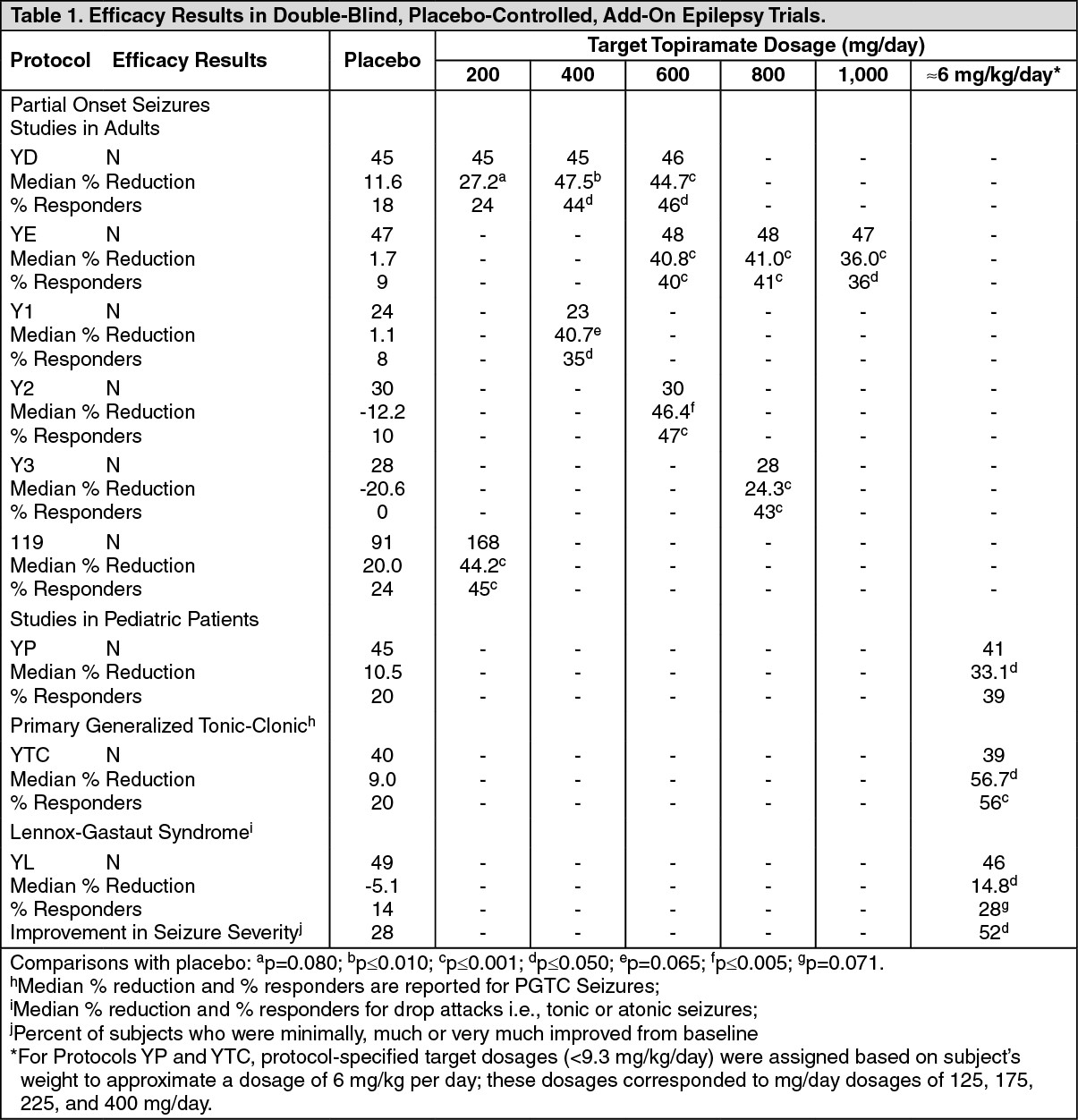
Patients in this study were permitted a maximum of two AEDs in addition to TOPAMAX or placebo. Patients who were experiencing at least 60 seizures per month before study entry were stabilized on optimum dosages of their concomitant AEDs during a four week baseline phase. Following baseline, patients were randomly assigned to placebo or TOPAMAX in addition to their other AEDs. Active drug was titrated beginning at 1 mg/kg per day for a week; the dose was then increased to 3 mg/kg per day for one week then to 6 mg/kg per day. After titration, patients entered an 8-week stabilization period. The primary measures of effectiveness were the percent reduction in drop attacks and a parental global rating of seizure severity. In all add-on trials, the reduction in seizure rate from baseline during the entire double-blind phase was measured. The median percent reductions in seizure rates and the responder rates (fraction of patients with at least a 50% reduction) by treatment group for each study are shown in Table 1. As described previously, a global improvement in seizure severity was also assessed in the Lennox-Gastaut trial. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSubset analyses of the antiepileptic efficacy of TOPAMAX Tablets in these studies showed no differences as a function of gender, race, age, baseline seizure rate, or concomitant AED.
Migraine Clinical Trials: The clinical development program to evaluate the efficacy of TOPAMAX in prophylaxis of migraine included two multicenter, randomized, double-blind placebo-controlled, parallel group pivotal trials conducted in North America (MIGR-001 and MIGR-002). The primary efficacy endpoint was the reduction in migraine headache frequency, as measured by the change in 4-week migraine rate from the baseline phase to the double-blind treatment phase in each TOPAMAX treatment group compared to placebo in the intent to treat (ITT) population.
The pooled results of the two pivotal trials evaluating TOPAMAX doses of 50 (N=233), 100 (N=244) and 200 mg/day (N=228) found a median percent reduction in average monthly migraine period rate of 35%, 51% and 49% respectively, compared to 21% for the placebo group (N=229). The 100 and 200 mg/day of TOPAMAX were statistically better then placebo. Notably, 27% of patients administered TOPAMAX 100 mg/day achieved at least a 75% reduction in migraine frequency, whilst 52% achieved at least a 50% reduction.
An additional supportive study, MIGR-003, demonstrated that TOPAMAX 100mg/day was comparable in terms of efficacy to propranolol 160 mg/day. There was no statistically significant difference between the two groups in the primary efficacy endpoint.
Pharmacokinetics: The pharmacokinetic profile of topiramate compared to other AEDs shows a long plasma half-life, linear pharmacokinetics, predominantly renal clearance, absence of significant protein binding, and lack of clinically relevant active metabolites. Topiramate is not a potent inducer of drug metabolizing enzymes, can be administered without regard to meals, and routine monitoring of plasma topiramate concentrations is not necessary. In clinical studies, there was no consistent relationship between plasma concentrations and efficacy or adverse events.
Absorption: Topiramate is rapidly and well absorbed. Following oral administration of 100 mg topiramate to healthy subjects, a mean peak plasma concentration (Cmax) of 1.5 mcg/mL was achieved within 2 to 3 hours (Tmax). Based on the recovery of radioactivity from the urine the mean extent of absorption of a 100 mg oral dose of 14C-topiramate was at least 81%. There was no clinically significant effect of food on the bioavailability of topiramate.
Distribution: Generally, 13 to 17% of topiramate is bound to plasma protein. A low capacity binding site for topiramate in/on erythrocytes that is saturable above plasma concentrations of 4 mcg/mL has been observed. The volume of distribution varied inversely with the dose. The mean apparent volume of distribution was 0.80 to 0.55 L/kg for a single dose range of 100 to 1200 mg. An effect of gender on the volume of distribution was detected, with values for females circa 50% of those for males. This was attributed to the higher percent body fat in female patients and is of no clinical consequence.
Metabolism: Topiramate is not extensively metabolized (~20%) in healthy volunteers. It is metabolized up to 50% in patients receiving concomitant antiepileptic therapy with known inducers of drug metabolizing enzymes. Six metabolites, formed through hydroxylation, hydrolysis and glucuronidation, have been isolated, characterized and identified from plasma, urine and feces of humans. Each metabolite represents less than 3% of the total radioactivity excreted following administration of 14C-topiramate. Two metabolites, which retained most of the structure of topiramate, were tested and found to have little or no anticonvulsant activity.
Elimination: In humans, the major route of elimination of unchanged topiramate and its metabolites is via the kidney (at least 81% of the dose). Approximately 66% of a dose of 14C-topiramate was excreted unchanged in the urine within four days. Following twice a day dosing with 50 mg and 100 mg of topiramate the mean renal clearance was approximately 18 mL/min and 17 mL/min, respectively. There is evidence of renal tubular reabsorption of topiramate. This is supported by studies in rats where topiramate was co-administered with probenecid, and a significant increase in renal clearance of topiramate was observed. Overall, plasma clearance is approximately 20 to 30 mL/min in humans following oral administration.
Topiramate exhibits low intersubject variability in plasma concentrations and, therefore, has predictable pharmacokinetics. The pharmacokinetics of topiramate are linear with plasma clearance remaining constant and area under the plasma concentration curve increasing in a dose-proportional manner over a 100 to 400 mg single oral dose range in healthy subjects. Patients with normal renal function may take 4 to 8 days to reach steady-state plasma concentrations. The mean Cmax following multiple, twice a day oral doses of 100 mg to healthy subjects was 6.76 mcg/ml. Following administration of multiple doses of 50 mg and 100 mg of topiramate twice a day, the mean plasma elimination half-life was approximately 21 hours.
Use with Other AEDs: Concomitant multiple-dose administration of topiramate, 100 to 400 mg twice a day, with phenytoin or carbamazepine shows dose proportional increases in plasma concentrations of topiramate.
Special Populations: Pediatric (up to 12 years of age): The pharmacokinetics of topiramate in children, as in adults receiving add-on therapy, are linear, with clearance independent of dose and steady-state plasma concentrations increasing in proportion to dose. Children, however, have a higher clearance and a shorter elimination half-life. Consequently, the plasma concentrations of topiramate for the same mg/kg dose may be lower in children compared to adults. As in adults, hepatic enzyme inducing AEDs decrease the steady-state plasma concentrations.
Elderly: Plasma clearance of topiramate is unchanged in elderly subjects in the absence of underlying renal disease.
Renal Impairment: The plasma and renal clearance of topiramate are decreased in patients with impaired renal function (CLCR <70 mL/min), and the plasma clearance is decreased in patients with end-stage renal disease. As a result, higher steady-state topiramate plasma concentrations are expected for a given dose in renally-impaired patients as compared to those with normal renal function.
Topiramate is effectively removed from plasma by hemodialysis.
Hepatic Impairment: Plasma clearance of topiramate is decreased in patients with moderate to severe hepatic impairment.
Toxicology: Preclinical Safety Data: Acute and long-term exposure of mice, rats, dogs and rabbits to topiramate was well tolerated. Hyperplasia of the gastric epithelial cells was observed only in rodents and in rats was reversible after 9 weeks without treatment.
Carcinogenicity and Mutagenicity: Tumors of smooth muscle origin in the urinary bladder were seen only in mice (oral dosages up to 300 mg/kg for 21 months) and appear to be unique to the species. Since no human counterpart exists, they were not considered clinically relevant. No such findings occurred in the rat carcinogenicity study (oral dosages up to 120 mg/kg/day for 24 months). Other toxicologic and pathologic effects of topiramate observed in these studies may be related to the weak induction of drug metabolizing enzymes or weak carbonic anhydrase inhibition.
In a battery of in vitro and in vivo mutagenicity assays, topiramate did not show genotoxic potential.
Reproductive and Developmental Toxicology: In preclinical studies, topiramate has been shown to have teratogenic effects in the species studied (mice, rats and rabbits). In mice, fetal weights and skeletal ossification were reduced at 500 mg/kg/day in conjunction with maternal toxicity. Overall numbers of fetal malformations in mice were increased for all drug-treated groups (20, 100 and 500 mg/kg/day), but no significant differences or dosage-response relationships were observed for overall or specific malformations, suggesting that other factors such as maternal toxicity may be involved.
In rats, dosage-related maternal and embryo/fetal toxicity (reduced fetal weights and/or skeletal ossification) were observed down to 20 mg/kg/day with teratogenic effects (limb and digit defects) at 400 mg/kg/day and above. In rabbits, dosage-related maternal toxicity was noted down to 10 mg/kg/day with embryo/fetal toxicity (increased lethality) down to 35 mg/kg/day, and teratogenic effects (rib and vertebral malformations) at 120 mg/kg/day.
The teratogenic effects seen in rats and rabbits were similar to those seen with carbonic anhydrase inhibitors, which have not been associated with malformations in humans. Effects on growth were also indicated by lower weights at birth and during lactation for pups from female rats treated with 20 or 100 mg/kg/day during gestation and lactation. In rats, topiramate crosses the placental barrier.
In juvenile rats, daily oral administration of topiramate at doses up to 300 mg/kg/day during the period of development corresponding to infancy, childhood, and adolescence resulted in toxicities similar to those in adult animals (decreased food consumption with decreased body weight gain, centrolobullar hepatocellular hypertrophy and slight urothelial hyperplasia in the urinary bladder). There were no relevant effects on long bone (tibia) growth or bone (femur) mineral density, preweaning and reproductive development, neurological development (including assessments on memory and learning), mating and fertility or hysterotomy parameters.
Fertility: Despite maternal and paternal toxicity as low as 8 mg/kg/day, no effects on fertility were observed, in male or female rats with up to 100 mg/kg/day.