Atorvastatin, fenofibrate.
Each tablet contains fixed dose combination of Atorvastatin Calcium USP equivalent to Atorvastatin 10 mg and Fenofibrate BP 160 mg.
Atorvastatin calcium is a synthetic lipid-lowering agent. Atorvastatin is an inhibitor of 3- hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase. This enzyme catalyzes the conversion of HMG-CoA to mevalonate, an early and rate-limiting step in cholesterol biosynthesis.
Atorvastatin calcium is [R-(R',R')]-2-(4-fluorophenyl)-β,δ-1.6-dihydroxy-5-(1-methylethyl)-3-phenyl-4(phenylamino) carbonyl]-1H-pyrrole-l-heptanoic acid, calcium salt (2:1) trihydrate.
The empirical formula of Atorvastatin calcium is (C33H34FN2O5)2Ca•3H2O and its molecular weight is 1209.42.
Fenofibrate is a lipid regulating agent available as tablets for oral administration. Each tablet contains 160 mg of fenofibrate. The chemical name for fenofibrate is 2-[4-(4-chlorobenzoyl) phenoxy]-2-methyl-propanoic acid, 1-methylethyl ester.
The empirical formula is C20H21O4Cl and the molecular weight is 360.83.
Excipients/Inactive Ingredients: Calcium carbonate, Lactose, Microcrystalline cellulose, Sodium Starch Glycolate, Hydroxypropyl cellulose, Magnesium stearate, Pregelatinised Starch, Croscarmellose Sodium, Crospovidone, Povidone, Sodium Lauryl Sulphate, Purified Talc, Colloidal anhydrous Silica. Colour: Ferric Oxide USP/NF (red).
Pharmacology: Pharmacodynamics: Mechanism of Action: Atorvastatin: Atorvastatin is a selective competitive inhibitor of 3-hydroxy-3-methyl-glutarylcoenzyrne A (HMG-CoA) reductase enzyme. This enzyme catalyzes the conversion of HMG-CoA to mevalonate, an early and rate limiting step in the synthesis of cholesterol.
The primary site of action of HMG-CoA reductase inhibitors is the liver. Inhibition of cholesterol synthesis in the liver leads to upregulation of low density lipoprotein (LDL) receptors and an increase in LDL-catabolism. There is also some reduction of LDL-production as a result of inhibition of hepatic synthesis of very low density lipoprotein (VLDL), the precursor of LDL-cholesterol. Atorvastatin reduces total cholesterol, LDL-cholesterol and apolipoprotein (apo) B in patients with homozygous and heterozygous familial hypercholesterolemia, non familial forms of hypercholesterolemia and mixed dyslipidemias. Atorvastatin also reduces VLDL-cholesterol and triglycerides and produces variable increases in high density lipoprotein (HDL)-cholesterol and apo AI. Atorvastatin reduces total cholesterol, LDL-cholesterol, VLDL-cholesterol, apo B, triglycerides, and non-HDL-cholesterol, and increases HDL-cholesterol in patients with isolated hypertriglyceridemia. Atorvastatin also reduces intermediate density lipoprotein (IDL) cholesterol in patients with dysbetalipoproteinemia.
Atorvastatin as well as some of its metabolites are pharmacologically active in humans. Drug dosage rather than systemic drug concentration correlates better with LDL-cholesterol reduction. Individualization of drug dosage should be based on therapeutic response.
Fenofibrate: Fenofibrate is a lipid regulating agent. Fenofibric acid, the active metabolite of fenofibrate, produces reductions in total-C, LDL-C, apo B, total triglycerides and VLDL in treated patients. In addition, treatment with fenofibrate results in increases in HDL-C and apoproteins apo AI and apo AII. The effects of fenofibric acid seen in clinical practice have been explained by the activation of peroxisome proliferator activated receptor (alpha) [PPAR (alpha)]. Through this mechanism, fenofibrate increases lipolysis and elimination of triglyceride-rich particles from plasma by activating lipoprotein lipase and reducing production of apoprotein C-III (an inhibitor of lipoprotein lipase activity). The resulting fall in triglycerides produces an alteration in the size and composition of LDL from small, dense particles (which are thought to be atherogenic due to their susceptibility to oxidation) to large buoyant particles. These larger particles have a greater affinity for cholesterol receptors and are catabolized rapidly. Activation of PPAR (alpha) also induces an increase in the synthesis of apoproteins A-I, A-II and HDL-cholesterol.
Fenofibrate also reduces serum uric acid levels in hyperuricemic and normal individuals by increasing the urinary excretion of uric acid.
Pharmacokinetics: Atorvastatin: Absorption: Atorvastatin is rapidly absorbed after oral administration; maximum plasma concentrations occur within 1 to 2 hours. Extent of absorption increases in proportion to atorvastatin dose. The absolute bioavailability of atorvastatin (parent drug) is approximately 14% and the systemic availability of HMG-CoA reductase inhibitory activity is approximately 30%. The low systemic availability is attributed to presystemic clearance in gastrointestinal mucosa and/or hepatic first-pass metabolism. Although food decreases the rate and extent of drug absorption by approximately 25% and 9%, respectively, as assessed by peak concentration (Cmax) and area under the curve (AUC), LDL-C reduction is similar whether atorvastatin is given with or without food. Plasma atorvastatin concentrations are lower (approximately 30% for Cmax and AUC) following evening drug administration compared with morning. However, LDL-C reduction is the same regardless of the time of day of drug administration.
Distribution: Mean volume of distribution of atorvastatin is approximately 381 liters. Atorvastatin is >98% bound to plasma proteins. A blood/plasma ratio of approximately 0.25 indicates poor drug penetration into red blood cells. Based on observations in rats, atorvastatin is likely to be secreted in human milk.
Metabolism: Atorvastatin is extensively metabolized to ortho-and parahydroxylated derivatives and various beta-oxidation products. In vitro inhibition of HMG-CoA reductase by ortho- and parahydroxylated metabolites is equivalent to that of atorvastatin. Approximately 70% of circulating inhibitory activity for HMG-CoA reductase is attributed to active metabolites. In vitro studies suggest the importance of atorvastatin metabolism by cytochrome P450 3A4, consistent with increased plasma concentrations of atorvastatin in humans following co-administration with erythromycin, a known inhibitor of this isozyme. In animals, the ortho-hydroxy metabolite undergoes further glucuronidation.
Excretion: Atorvastatin and its metabolites are eliminated primarily in bile following hepatic and/or extra-hepatic metabolism; however, the drug does not appear to undergo enterohepatic recirculation. Mean plasma elimination half-life of atorvastatin in humans is approximately 1-4 hours, but the half-life of inhibitory activity for HMG-CoA reductase is 20 to 30 hours due to the contribution of active metabolites. Less than 2% of a dose of atorvastatin is recovered in urine following oral administration.
Special Populations: Geriatric: Plasma concentrations of atorvastatin are higher (approximately 40% for Cmax and 30% for AUC) in healthy elderly subjects (age >65 years) than in young adults. Clinical data suggest a greater degree of LDL-lowering at any dose of drug in the elderly patient population compared to younger adults.
Pediatric: Pharmacokinetic data in the pediatric population are not available.
Gender: Plasma concentrations of atorvastatin in women differ from those in men (approximately 20% higher for Cmax and 10% lower for AUC); however, there is no clinically significant difference in LDL-C reduction with atorvastatin between men and women.
Renal Impairment: Renal disease has no influence on the plasma concentrations or LDL-C reduction of atorvastatin; thus, dose adjustment in patients with renal dysfunction is not necessary.
Hemodialysis: While studies have not been conducted in patients with end-stage renal disease, hemodialysis is not expected to significantly enhance clearance of atorvastatin since the drug is extensively bound to plasma proteins.
Hepatic Impairment: In patients with chronic alcoholic liver disease, plasma concentrations of atorvastatin are markedly increased. Cmax and AUC are each 4-fold greater to patients with Childs-Pugh A disease. Cmax and AUC are approximately 16-fold and 11-fold increased, respectively, in patients with Childs-Pugh B disease.
Fenofibrate: Absorption: After fenofibrate is dissolved, fenofibrate is well absorbed from the gastrointestinal tract. Its bioavailability is optimized when taken with meals.
Distribution: In healthy volunteers administered formulation of fenofibrate, steady-state plasma levels of fenofibric acid were shown to be achieved within 5 days of daily dosing with single oral doses and did not demonstrate accumulation across time following multiple dose administration. Serum protein binding was approximately 99% bound to plasma proteins in normal and hyperlipidemic subjects.
Metabolism: Following oral administration, fenofibrate is rapidly hydrolyzed by esterases to the active metabolite, fenofibric acid; no unchanged fenofibrate is detected in plasma of healthy subjects following fenofibrate administration. Fenofibric acid is primarily conjugated with glucuronic acid and then excreted in urine. A small amount of fenofibric acid is reduced at the carbonyl moiety to a benzhydrol metabolite which is, in turn, conjugated with glucuronic acid and excreted in urine.
In vivo metabolism data indicate that neither fenofibrate nor fenofibric acid undergo oxidative metabolism (e.g., cytochrome P450) to a significant extent.
Excretion: After absorption, fenofibrate is mainly excreted in the urine in the form of metabolites, primarily fenofibric acid and fenofibric acid glucuronide. After administration of radiolabeled fenofibrate, approximately 60% of the dose appeared in the urine and 25% was excreted in the feces. Fenofibric acid is eliminated with a half-life of approximately 16 hours, allowing once daily administration in a clinical setting.
Special Populations: Geriatrics: A study using formulation of fenofibrate shows that the oral clearance of fenofibric acid is similar to that of young adults. This indicates that a similar dosage regimen can be used in the elderly, without increasing accumulation of the drug or metabolites.
Pediatrics: Fenofibrate has not been investigated in adequate and well-controlled trials in pediatric patients.
Gender: No pharmacokinetic difference between males and females has been observed for fenofibrate.
Renal Impairment: In a study using formulation in patients with severe renal impairment (creatinine clearance <50 mL/min), the rate of clearance of fenofibric acid was greatly reduced, and the compound accumulated during chronic dosage. However, in patients having moderate renal impairment (creatinine clearance of 50 to 90 mL/min), the oral clearance and the oral volume of distribution of fenofibric acid are increased compared to healthy adults. Therefore, the dosage of fenofibrate should be minimized in patients who have severe renal impairment, while no modification of dosage is required in patients having moderate renal impairment.
Hepatic Impairment: No pharmacokinetic studies have been conducted in patients with hepatic insufficiency.
Combined hyperlipidemia: Tonact-FN is indicated as an adjunct to diet to reduce elevated total-C, LDL-C, apo B. and TG levels and to increase HDL-C in these patients.
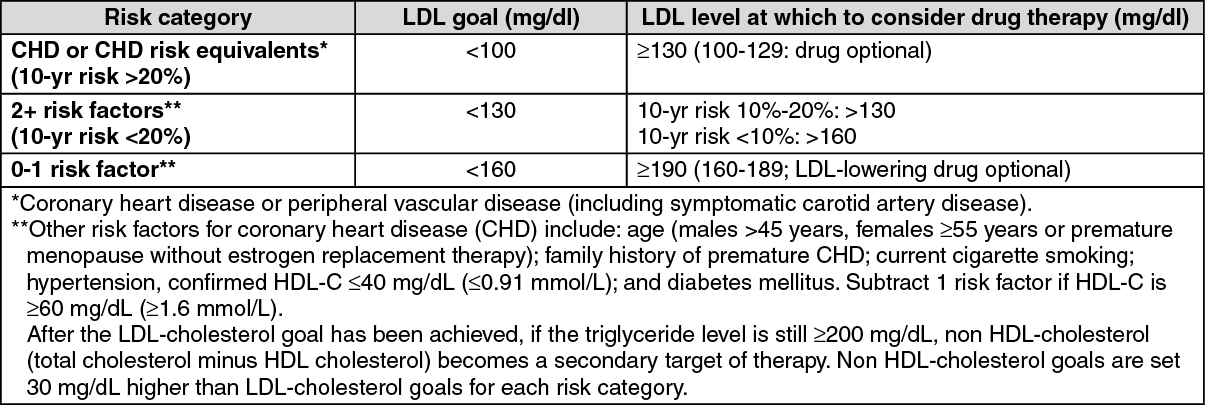
Lipid altering agents should be used in addition to diet restricted in saturated fat and cholesterol only when the response to diet and other non pharmacological measures has been inadequate (see National Cholesterol Education Program (NCEP) Guidelines, summarized in the table).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patients should be placed on an appropriate lipid-lowering diet before receiving Tonact-FN, and should continue this diet during treatment. Tonact-FN should be given with meals. thereby optimizing the bioavailability of the medication.
The recommended dosage is one tablet once daily.
Dosage in Patients Taking Cyclosporine, Clarithromycin or a Combination of Ritonavir plus Saquinavir or Lopinavir plus Ritonavir: In patients taking cyclosporine, therapy should be limited to atorvastatin 10 mg once daily. In patients taking clarithromycin or in patients with HIV taking a combination of ritonavir plus saquinavir or lopinavir plus ritonavir, for doses of atorvastatin exceeding 20 mg appropriate clinical assessment is recommended to ensure that the lowest dose necessary of atorvastatin is employed.
Administration: The route of administration is oral.
Atorvastatin: There is no specific treatment available for atorvastatin overdosage. General supportive measures should be adopted as required. Liver function tests and serum CPK levels should be monitored. Due to extensive drug binding to plasma proteins, haemodialysis is not expected to significantly enhance atorvastatin clearance.
Fenofibrate: There is no specific treatment for overdose with fenofibrate. General supportive care of the patient is indicated, including monitoring of vital signs and observation of clinical status, should an overdose occur. If indicated, elimination of unabsorbed drug should be achieved by emesis or gastric lavage; usual precautions should be observed to maintain the airway. Because fenofibrate is highly bound to plasma proteins, hemodialysis should not be considered.
Hypersensitivity to either component.
Hepatic or severe renal dysfunction, including primary biliary cirrhosis, and patients with unexplained persistent liver function abnormality.
Unexplained persistent elevations of serum transaminases exceeding three times the upper limit of normal.
Preexisting gallbladder disease.
Pregnancy and lactation.
It is recommended that liver function tests should be done before initiation of Tonact-FN therapy, at 12 weeks after initiation of therapy and periodically thereafter semiannually. If the liver enzyme values exceed three times the upper normal limit, Tonact-FN must be discontinued. If cholelithiasis is suspected, or if gallstones are found, fenofibrate (in Tonact-FN) must be stopped.
Combined use of oral anticoagulants, cyclosporine and resins with fenofibrate (in Tonact-FN) should be with due precaution. Medications known to exacerbate hypertriglyceridemia (beta blockers, thiazides, estrogens) should be discontinued or changed if possible prior to consideration of fenofibrate (in Tonact-FN) therapy.
Safety and efficacy of fenofibrate and atorvastatin (in Tonact-FN) in pediatric patients have not been established. Dose of fenofibrate (in Tonact-FN) must be carefully titrated in the elderly.
Tonact-FN must be preferably avoided in those with any evidence of hepatic disease, or those consuming substantial quantities of alcohol. Fenofibrate (in Tonact-FN) is to be given with care in the presence of pancreatitis.
Tonact-FN should be discontinued, or temporarily withheld, in any patient with an acute, serious condition suggestive of myopathy or having a risk factor predisposing to the development of renal failure secondary to rhabdomyolysis (e.g. severe acute infection, hypotension, major surgery, trauma, severe metabolic, endocrine and electrolyte disorders, and uncontrolled seizures). Myopathy should be considered in any patients with diffuse myalgias, muscle tenderness or weakness, and/or marked elevation of creatine phosphokinase.
Liver function: The two drugs, given individually, have been associated with biochemical abnormalities of liver function. Persistent elevations (>3 times the upper limit of normal [ULN] occurring on two or more occasions) in serum transaminases occurred in 0.7% of patients who received atorvastatin in clinical trials. Specifically, the incidence of these abnormalities was 0.2% for atorvastatin 10 mg.
In a pooled analysis of 10 placebo-controlled trials, increases in serum transaminases to >3 ULN occurred in 5.3% of patients taking fenofibrate versus 1.1% of patients treated with placebo.
It is recommended that liver function tests be performed prior to and at 12 weeks following initiation of therapy and periodically thereafter (eg semiannually). Patients who develop increased transaminase levels should be monitored until the abnormalities resolve. Should an increase in ALT or AST of >3 times ULN persist, withdrawal of Tonact-FN is recommended. Tonact-FN should be used with caution in patients who consume substantial quantities of alcohol and/or have a past history of liver disease.
Skeletal muscle: The use of Tonact-FN may occasionally be associated with myopathy since the two drugs, individually, have been shown to cause myopathy in a small percentage of patients (<1%) in international trials.
Treatment with atorvastatin as well as fenofibrate has been associated on rare occasions with rhabdomyolysis, usually in patients with impaired renal function. Myopathy should be considered in any patient with diffuse myalgias, muscle tenderness or weakness, and/or marked elevations of CPK levels. The risk of myopathy during treatment may be increased with concurrent administration of cyclosporin, erythromycin, niacin or azole anti-fungals. Patients should be advised to report promptly unexplained muscle pain, tenderness or weakness, particularly if accompanied by malaise or fever. The CPK levels should be assessed in patients reporting these symptoms and Tonact-FN therapy should be discontinued if markedly elevated CPK levels occur or myopathy is diagnosed.
Tonact-FN therapy should be temporarily withheld or discontinued in any patient with acute, serious condition suggestive of a myopathy or having a risk factor predisposing to the development of renal failure secondary to rhabdomyolysis (eg. severe acute infection, hypotension, major surgery, trauma, severe metabolic, endocrine and electrolyte disorders, and uncontrolled seizures).
Endocrine Function: Statins interfere with cholesterol synthesis and theoretically might blunt adrenal and/or gonadal steroid production. Clinical studies have shown that atorvastatin does not reduce basal plasma cortisol concentration or impair adrenal reserve. The effects of statins on male fertility have not been studied in adequate numbers of patients. The effects, if any, on the pituitary-gonadal axis in premenopausal women are unknown. Caution should be exercised if Tonact-FN is administered concomitantly with drugs that may decrease the levels or activity of endogenous steroid hormones, such as ketoconazole, spironolactone and cimetidine.
Cholelithiasis: Fenofibrate may increase cholesterol excretion into the bile, leading to cholelithiasis. If cholelithiasis is suspected, gallbladder studies are indicated. Tonact-FN therapy should be discontinued if gallstones are found.
Pancreatitis: Pancreatitis has been reported in patient taking fenofibrate. This occurrence may represent a failure of efficacy in patients with severe hypertriglyceridemia, a direct drug effect, or a secondary phenomenon mediated through biliary tract stone or sludge formation with obstruction of the common bile duct.
Renal Impairment: Renal disease has no influence on the plasma concentrations or lipid effects of atorvastatin. However, fenofibric acid is known to be substantially excreted by the kidney and the risk of adverse reactions may be greater in patients with impaired renal function. Tonact-FN is not recommended for use in patients with severe renal impairment.
Hepatic impairment: In patients with chronic alcoholic liver disease, the therapeutic response to atorvastatin is unaffected but exposure to the drug is greatly increased. Therefore, caution should be exercised in patients who consume substantial quantities of alcohol and/or have a history of liver disease. As atorvastatin is contraindicated, Tonact-FN cannot be used in patients with active liver disease which may include unexplained persistent elevations in hepatic transaminase levels.
Pediatric Use: Safety and efficacy of atorvastatin-fenofibrate combination in pediatric patients have not been established.
Pregnancy: Since statins decrease cholesterol synthesis and possibly the synthesis of other biologically active substances derived from cholesterol, they may cause fetal harm when administered to the pregnant woman. Tonact-FN is therefore contraindicated during pregnancy. Tonact-FN should be administered to women of childbearing age only when such patients are highly unlikely to conceive and have been informed of the potential hazards. If the patient becomes pregnant while taking this drug, therapy should be discontinued and the patients apprised of the potential hazard to the fetus.
Lactation: Tonact-FN is contraindicated in nursing mothers. Because of the potential for adverse reactions in nursing infants, women taking Tonact-FN should not breast-feed.
The combination of atorvastatin and fenofibrate is generally well tolerated. In studies conducted with Tonact-FN (n=82), the reported side effects were gastritis (2%), leg pain (6%), burning feet (2%), body ache (6%), numbness in legs (4%), joint pain (1%), pruritus (1%), hyperglycemia (1%) and dizziness (2%). All these effects were mild and transient.
Other side effects with the combination may include nausea, headache, abdominal pain, constipation, dyspepsia, flatulence, diarrhea, dizziness, insomnia, hepatitis, cholelithiasis, cholecystitis, hepatomegaly, photosensitivity, myopathy, rhabdomyolysis and eczema.
Strong Inhibitors of CYP3A4: Atorvastatin is metabolized by CY3A4. Concomitant administration of atorvastatin with strong inhibitors of CYP3A4 (clarithromycin, combination of protease inhibitors, itraconazole, diltiazem hydrochloride) can lead to increases in plasma concentrations of atorvastatin. The extent of interaction and potentiation of effects depends on the variability of effect on CYP3A4.
Inducers of CYP3A4: Concomitant administration of atorvastatin with inducers of CYP34 (eg efavirenz, rifampin) can lead to variable reductions in plasma concentrations of atorvastatin. Due to the dual interaction mechanism of rifampin, simultaneous co-administration of atorvastatin with rifampin is recommended, as delayed administration of atorvastatin after administration of rifampin has been associated with a significant reduction in atorvastatin plasma concentrations.
Erythromycin: In healthy individual, plasma concentrations of atorvastatin increased by approximately 40% with coadministration of atorvastatin and erythromycin, a known inhibitor of cytochrome P450 3A4. The risk of myopathy is increased when statins and erythromycin are concurrently administered. Caution should be exercised when coadministering Tonact-FN with erythromycin.
Colestipol: Plasma concentrations of atorvastatin decreased approximately 25% when colestipol and atorvastatin were coadministered. However, LDL-C reduction was greater when atorvastatin and colestipol were coadministered than when either drug was given alone. Since bile acid sequestrants may bind other drugs given concurrently, patients should take Tonact-FN at least 1 hour before or 4-6 hours after a bile acid binding resin to avoid impending its absorption.
Digoxin: Administration of multiple doses of atorvastatin with digoxin increases the steady-state plasma digoxin concentrations by approximately 20%. Patients taking digoxin and Tonact-FN concomitantly should be monitored appropriately.
Oral Contraceptives: Co administration of atorvastatin and an oral contraceptive containing norethindrone and ethinyl estradiol produces increased plasma concentrations of norethindrone and ethinyl estradiol. These increases should be considered when selecting an oral contraceptive for a woman taking Tonact-FN.
Oral Anticoagulants: If coumarin anticoagulants and Tonact-FN are co administered, the dosage of the anticoagulant should be reduced to maintain the prothrombin time/INR at the desired level to prevent bleeding complications. Frequent prothrombin time/INR determinations are advisable until it has been definitely determined that the prothrombin time/INR has stabilized.
Cyclosporine: Because cyclosporine can produce nephrotoxicity with decreases in creatinine clearance and rises in serum creatinine, and because renal excretion is the primary elimination route of fibrate drugs including fenofibrate, there is a risk that an interaction will lead to deterioration. The benefits and risk of using Tonact-FN with immunosuppressants and other potentially nephrotoxic agents should be carefully considered. Also, the risk of myopathy during treatment with statins is increased with concurrent administration of cyclosporine. Hence, caution should be exercised when coadministering Tonact-FN with cyclosporine.
Azole antifungals/Niacin: The risk of myopathy during treatment with statins is increases with concurrent administration of these agents. Hence caution should be exercised when these drugs are coadministered with Tonact-FN.
Store below 25°C. Protect from light and moisture.
Shelf-Life: 24 months.
C10BA - Combinations of various lipid modifying agents ; Used in the treatment of hyperlipidemia.
Tab [capsule shaped, biconvex, bevelled edge, uncoated bilayered, with one layer white in colour (Fenofibrate layer) and other layer light brick red in colour (Atorvastatin layer), plain on both sides] x 10 x 10's.



 Sign Out
Sign Out