Adult: 200 mg bid. Max: 400 mg daily. Usual treatment duration: 7 days. Use the lowest effective dose for the shortest possible duration. Dosage is adjusted according to individual patient needs and response. Elderly: Use the lowest effective dose for the shortest possible duration.
Adult: Initially, 150 mg or 200 mg bid. Max: 400 mg daily. Use the lowest effective dose for the shortest possible duration. Dosage is adjusted according to individual patient needs and response. Elderly: Use the lowest effective dose for the shortest possible duration.
Adult: 200 mg bid. Max: 400 mg daily. Usual treatment duration: 7-14 days. Use the lowest effective dose for the shortest possible duration. Dosage is adjusted according to individual patient needs and response. Elderly: Use the lowest effective dose for the shortest possible duration.
Renal Impairment
Dosage reduction may be necessary. Severe: Contraindicated. Treatment recommendations may vary among countries and individual products (refer to detailed product guideline).
Hepatic Impairment
Dosage reduction may be necessary. Severe: Contraindicated. Treatment recommendations may vary among countries and individual products (refer to detailed product guideline).
Administration
Should be taken with food.
Contraindications
Hypersensitivity; history of asthma, urticaria, or allergic-type reactions after aspirin or other NSAID use. Active or history of recurrent gastrointestinal ulceration or bleeding (≥2 distinct episodes of proven ulceration or bleeding); history of gastrointestinal bleeding or perforation associated with previous NSAID therapy; severe heart failure. Use in the setting of CABG surgery. Severe renal and hepatic impairment. Pregnancy (3rd trimester).
Special Precautions
Patient with history of ulcerative colitis or Crohn's disease; hypertension, mild to moderate CHF, recent MI, other forms of asthma, hypovolaemia, oedema, ischaemic heart disease, peripheral arterial disease, cerebrovascular disease; coagulopathy, diabetes; SLE, mixed connective tissue disorder; history of renal lithiasis. Use may mask the usual signs and symptoms of infection. Avoid concomitant use with other NSAIDs (including cyclooxygenase-2 inhibitors). Smokers. Dehydrated or debilitated patients. Elderly. Mild to moderate renal and hepatic impairment. Pregnancy (1st to 2nd trimester) and lactation.
Adverse Reactions
Significant: Anaphylactoid reactions, new-onset or exacerbation of hypertension, Na and fluid retention, aseptic meningitis, anaemia, transaminase elevations, pancreatitis, hyperkalaemia; oedema; decreased platelet adhesion and aggregation, prolonged bleeding time; renal decompensation (usually reversible); renal papillary necrosis (long-term use), renal calculi, acute interstitial nephritis with haematuria, proteinuria, and occasionally, nephrotic syndrome. Rarely, severe blood dyscrasias (e.g. agranulocytosis, thrombocytopenia, aplastic anaemia). Ear and labyrinth disorders: Tinnitus. Gastrointestinal disorders: Nausea, vomiting, gastrointestinal cramps or pain, diarrhoea, constipation, flatulence, dyspepsia. Metabolism and nutrition disorders: Anorexia. Nervous system disorders: Dizziness, headache, nervousness. Skin and subcutaneous tissue disorders: Rash, pruritus. Potentially Fatal: CV thrombotic events, including MI and stroke (increased risk with higher doses and prolonged use); gastrointestinal bleeding, ulceration, and perforation; drug reaction with eosinophilia and systemic symptoms (DRESS)/multiorgan hypersensitivity reactions, exfoliative dermatitis, Stevens-Johnson syndrome, toxic epidermal necrolysis. Rarely, severe hepatic reactions (e.g. fulminant hepatitis, hepatic necrosis, hepatic failure).
PO: C, Z (NSAIDs caused foetal ductus arteriosus premature closure, foetal renal impairment and persistent pulmonary hypertension. Avoid near term, else use lowest dose for shortest time.)
Patient Counseling Information
This drug may cause drowsiness, dizziness, or blurred vision, if affected, do not drive or operate machinery.
Monitoring Parameters
Assess cardiac risk and potential for gastrointestinal bleeding prior to initiation of therapy. Monitor blood pressure and signs and symptoms of gastrointestinal bleeding, hepatotoxicity, and ototoxicity at the start of therapy and periodically throughout use; CBC, chemistry profile, occult blood loss, periodic LFTs, renal function (e.g. urine output, serum BUN and creatinine). Perform ophthalmic evaluations if ocular complaints develop during treatment or prolonged use.
Overdosage
Symptoms: Headache, nausea, vomiting, epigastric pain, gastrointestinal pain and bleeding. Rarely, diarrhoea, disorientation, excitation, tinnitus, fainting, convulsions, stupor, decreased urine output, hypotension, coma, and death. Management: Symptomatic and supportive treatment. Induce vomiting or perform gastric lavage to empty stomach contents. May consider activated charcoal to decrease absorption and alkalinisation of the urine to enhance excretion. Administer diazepam for frequent or prolonged convulsions. Ensure good urine output. Monitor LFTs and renal function.
Drug Interactions
May decrease the therapeutic effect of ACE-inhibitors, angiotensin II antagonists, diuretics (e.g. furosemide, thiazide diuretics). Decreased serum concentration of the active metabolite of sulindac when given with aspirin, diflunisal, dimethyl sulfoxide. May reduce clearance and increase the risk of toxicity of lithium and methotrexate. Increased risk of gastrointestinal toxicity with other NSAIDs. Increased risk of gastrointestinal bleeding with oral anticoagulants (e.g. warfarin), antiplatelet agents, corticosteroids, and SSRIs. Increased serum concentration with probenecid. May increase the risk of nephrotoxicity with tacrolimus, ciclosporin, or diuretics. May increase the risk of haematological toxicity when given with zidovudine.
Lab Interference
May cause false-positive aldosterone/renin ratio (ARR).
Action
Description: Sulindac is an NSAID with analgesic and antipyretic properties. Its mechanism of action is not completely understood but it may be associated with the reversible inhibition of cyclooxygenase-1 and 2 (COX-1 and 2) enzymes, thereby causing a decreased formation of prostaglandin precursors. Onset: Within 1 week. Pharmacokinetics: Absorption: Absorbed from the gastrointestinal tract. Time to peak plasma concentration: Approx 3-4 hours (sulindac); approx 5-6 hours (sulfide and sulfone metabolites). Distribution: Crosses the placenta and blood-brain barrier (brain concentration: <4% of plasma concentrations). Plasma protein binding: 93.1% (sulindac); 97.9% (sulfide metabolite); 95.4% (sulfone metabolite); primarily to albumin. Metabolism: Metabolised in the liver via reduction to the sulfide metabolite (active) and via oxidation to the sulfone metabolite (inactive); undergoes extensive enterohepatic recirculation. Excretion: Via urine (approx 50%, mainly as sulfone metabolite and its glucuronide conjugate; <1% as sulfide metabolite); faeces (approx 25%, mainly as sulfone and sulfide metabolites). Elimination half-life: 7.8 hours (sulindac); 16.4 hours (sulfide metabolite).
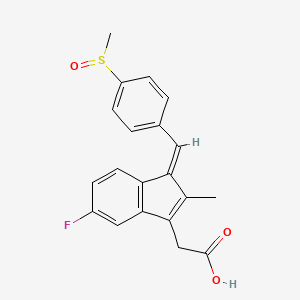
Chemical Structure
Sulindac Source: National Center for Biotechnology Information. PubChem Compound Summary for CID 1548887, Sulindac. https://pubchem.ncbi.nlm.nih.gov/compound/Sulindac. Accessed Feb. 23, 2022.
M01AB02 - sulindac ; Belongs to the class of acetic acid derivatives and related substances of non-steroidal antiinflammatory and antirheumatic products.
References
Anon. Sulindac. AHFS Clinical Drug Information [online]. Bethesda, MD. American Society of Health-System Pharmacists, Inc. https://www.ahfscdi.com. Accessed 27/12/2021.Anon. Sulindac. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 14/12/2021.Buckingham R (ed). Sulindac. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 14/12/2021.Joint Formulary Committee. Sulindac. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 14/12/2021.Sulindac 100 mg Tablets (Chemidex Pharma Limited t/a Essential Generics). MHRA. https://products.mhra.gov.uk. Accessed 14/12/2021.Sulindac 200 mg Tablets (Chemidex Pharma Limited t/a Essential Generics). MHRA. https://products.mhra.gov.uk. Accessed 14/12/2021.Sulindac Tablet (Watson Pharma Private Limited). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed. Accessed 14/12/2021.



 Sign Out
Sign Out