Renal Insufficiency: In cases of severe renal insufficiency (creatinine clearance <30 mL/min), the treatment is contraindicated.
In certain hypersensitive patients without preexisting apparent renal lesion and for whom the biology screen shows a functional renal insufficiency, the treatment should be stopped and possibly restarted either at a low dose or with one constituent only.
In these patients, the normal medical practice includes periodic control for potassium and creatinine after 2 weeks of treatments and then every 2 months during therapeutic stability period.
Preterax 2.5 mg: Renal insufficiency has been reported mainly in patients using Preterax 2.5 mg with severe cardiac insufficiency or renal insufficiency with renal artery stenosis.
Preterax 5 mg: In cases of renal insufficiency (creatinine clearance <60 mL/min), the dosage is reduced.
In such patients and in those suffering from glomerular nephropathy, normal medical practice includes periodic testing of potassium and creatinine levels (see Dosage & Administration).
Hypotension and Salt and Water Depletion: There is a risk of sudden hypotension in subjects with preexisting sodium depletion (particularly in patients presenting with renal artery stenosis). Therefore, systematic testing should be carried out for the clinical signs of salt and water depletion, which may occur with an intercurrent episode of diarrhoea or vomiting. Regular monitoring of plasma electrolytes should be carried out in such patients.
Marked hypotension may require the implementation of an IV infusion of isotonic saline.
Transient hypotension is not a contraindication for continuation of treatment. After re-establishment of a satisfactory blood volume and blood pressure, treatment can be started again either at a reduced dose or with only one of the constituents.
Potassium Levels: The combination of perindopril and indapamide does not prevent the onset of hypokalaemia in particular in diabetic patients or in patients with renal failure. As with any antihypertensive agent containing a diuretic, regular monitoring of plasma potassium levels should be carried out.
Linked to Perindopril: Cough: A dry cough has been reported with the use of angiotensin-converting enzyme inhibitors. It is characterised by its persistence and by its disappearance when treatment is withdrawn. An iatrogenic aetiology should be considered on the event of this symptom. If the prescription of an angiotensin-converting enzyme inhibitor is judged indispensable, continuation of treatment may be considered.
Risk of Arterial Hypotension and/or Renal Insufficiency (In Cases of Cardiac Insufficiency, Salt and Water Depletion, Etc): Marked stimulation of the renin-angiotensin-aldosterone system has been observed particularly during marked salt and water depletion (strict sodium-free diet or prolonged diuretic treatment), in patients whose blood pressure was initially low, in cases of renal arterial stenosis, congestive heart failure or cirrhosis with oedema and ascites.
The blocking of this system with an angiotensin-converting enzyme inhibitor may therefore cause a sudden drop in blood pressure, particularly at the time of the 1st administration and during the first 2 weeks of treatment and/or an increase in plasma levels of creatinine, showing a functional renal insufficiency which is sometimes acute, although this is rare and the time to onset varies more.
In all cases of this type, the treatment should then be initiated at a lower dose and increased progressively.
Patients with Known Atherosclerosis: As the risk of hypotension exists in all patients, particular care should be taken in patients with ischaemic heart disease or cerebral circulatory insufficiency, with treatment being started at a low dose.
Renovascular Hypertension: The treatment for renovascular hypertension is revascularization. Nonetheless, angiotensin-converting enzyme inhibitors can be beneficial in patients presenting with renovascular hypertension who are awaiting corrective surgery or when such a surgery is not possible.
Treatment should then be started in a hospital at a low dose and renal function and potassium levels should be monitored, since some patients have developed a functional renal insufficiency which is reversible when treatment is stopped.
Other Populations at Risk: In patients with severe cardiac insufficiency (grade IV) or in patients with insulin dependent diabetes mellitus (spontaneous tendency to increased levels of potassium), treatment should be started under medical supervision with a reduced initial dose. Treatment with β-blockers in hypertensive patients with coronary insufficiency should not be stopped: the ACE inhibitor should be added to the β-blocker.
Anaemia: Anaemia has been observed in patients who have had a kidney transplant or have been undergoing dialysis, with a reduction in haemoglobin levels which is all the more marked since the initial values are high. This effect does not seem to be dose-dependent but may be linked to the mechanism of action of angiotensin-converting enzyme inhibitors.
This reduction is slight, occurs within 1-6 months, and then remains stable. It is reversible when treatment is stopped. Treatment can be continued in this type of patient, carrying out regular haematological testing.
Surgery: Angiotensin-converting enzyme inhibitors can cause hypotension in cases of anaesthesia, and particularly when the anaesthetic administered is an agent with hypotensive potential. It is therefore recommended that treatment with long-acting angiotensin-converting enzyme inhibitors eg, perindopril, should be discontinued where possible 2 days before surgery.
Aortic Stenosis/Hypertrophic Cardiomyopathy: Preterax 2.5 mg: Angiotensin-converting enzyme inhibitors must be used with care in patients presenting with left ventricular obstruction.
Linked to Indapamide: Salt and Water Balance: Sodium Levels: These should be tested before treatment is started, then at regular intervals. All diuretic treatment can cause a reduction in sodium levels, which may have serious consequences. The reduction in sodium level can be initially asymptomatic, and regular testing is therefore essential. Testing should be more frequent in risk populations eg, elderly and cirrhotic patients (see Adverse Reactions and Overdosage).
Potassium Levels: Potassium depletion with hypokalaemia is a major risk with thiazide diuretics and thiazide-related diuretics. The risk of onset of lowered potassium levels (<3.4 micromol/L) should be prevented in some at risk populations eg, elderly and/or malnourished subjects, whether or not they are taking multiple medications; cirrhotic patients with oedema and ascites; coronary patients and patients with heart failure.
In such cases, hypokalaemia increases the cardiac toxicity of cardiac glycosides and the risk of rhythm disorders.
Subjects presenting with a long QT interval are also at risk, whether the origin is congenital or iatrogenic. The hypokalaemia, as with bradycardia, acts as a factor which favours the onset of severe rhythm disorders, in particular Torsade de pointes, which may be fatal.
In all cases more frequent testing of potassium levels is necessary. The first measurement of plasma potassium levels should be carried out during the 1st week following the start of treatment.
If low potassium levels are detected, correction is required.
Calcium Levels: Thiazide diuretics and thiazide-related diuretics may reduce urinary excretion of calcium and cause a mild and transient increase in plasma calcium levels. Markedly raised levels of calcium may be related to undiagnosed hyperparathyroidism. In such cases, the treatment should be stopped before investigating the parathyroid function.
Blood Glucose: Monitoring of blood glucose is important in diabetic patients, particularly when potassium levels are low.
Uric Acid: Patients with raised levels of uric acid may have an increased tendency to gout attacks.
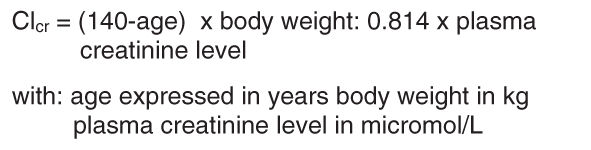
Renal Function and Diuretics: Thiazide diuretics and thiazide-related diuretics are only fully effective when renal function is normal or only slightly impaired (creatinine levels approximately <25 mg/L ie, 220 micromol/L for an adult).
In the elderly the value of plasma creatinine levels should be adjusted to take account of the age, weight and sex of the patient, according to the Cockcroft formula:
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Hypovolaemia, resulting from the loss of water and sodium caused by the diuretic at the start of treatment, causes a reduction in glomerular filtration. It may result in an increase in blood urea and creatinine levels. This transitory functional renal insufficiency is of no consequence in subjects with normal renal function but may however worsen a preexisting renal insufficiency.
Athletes: Athletes should note that Preterax contains an active substance which may cause a positive reaction in doping tests.
Lactose: Preterax 2.5 mg contains lactose and is, in consequence, contraindicated in the case of congenital galactosemia, glucose and galactose malabsorption or lactase deficiency syndrome (rare metabolic diseases).
Effects on the Ability to Drive or Operate Machinery: Linked to Perindopril, Indapamide and Preterax: Neither the 2 active substances nor Preterax affects alertness but individual reactions related to low blood pressure may occur in some patients, particularly at the start of treatment or in combination with another antihypertensive medication. As a result, the ability to drive or operate machinery may be impaired.
Use in pregnancy & lactation: Preterax 2.5 mg: The presence of an angiotensin-converting enzyme inhibitor determines the contraindication for the use of this combination during pregnancy and lactation.
Linked to Perindopril: Pregnancy: No appropriate and well-controlled studies have been carried out in humans. Angiotensin-converting enzyme inhibitors cross the placenta and may lead to foetal and neonatal morbidity and mortality when administered to pregnant women.
Cases of neonatal hypotension, renal insufficiency, malformations of the face and the cranial vault and/or death have been reported when the foetus is exposed during the 2nd and 3rd trimesters of pregnancy. A reduction in foetal renal function with maternal oligohydramnios has also been observed.
Contractions of the limbs, craniofacial malformations, pulmonary hypoplasia and intrauterine growth retardation with oligohydramnios have been reported.
Infants who were exposed to angiotensin-converting enzyme inhibitors
in utero should be carefully monitored for hypotension, oliguria and hyperkalaemia. Oliguria can be treated with support of blood pressure and renal blood flow.
Intrauterine growth retardation, prematurity, patent ductus arteriosus and foetal death have been reported, although no clear relationships with angiotensin-converting enzyme inhibitors or with maternal concomitant illness have been established.
No data are available on whether limited exposure in the 1st trimester of pregnancy affects the foetus.
If the patient becomes pregnant while taking an angiotensin-converting enzyme inhibitor, she must be informed of the potential risks to the foetus.
Lactation: Angiotensin-converting enzyme inhibitors can be excreted in breast milk and the effects on nursing infants are unknown. Breastfeeding is therefore contraindicated in women who are being treated with angiotensin-converting enzyme inhibitors.
Preterax 5 mg: As the combination includes an ACE inhibitor, Preterax 5 mg is contraindicated during pregnancy.
Pregnancy: Studies in animals have shown no teratogenic effects, but toxicity to the foetus was shown in several species.
In pregnant women receiving treatment with angiotensin-converting enzyme inhibitors, no epidemiological studies are available; isolated observations of pregnancies exposed in the 1st trimester are
a priori reassuring with regard to malformation, with the exception of some cases of abnormalities of the skull reported with the use of angiotensin-converting enzyme inhibitors throughout pregnancy; administration during the 2nd and 3rd trimesters, particularly if continued until delivery, produces a risk of renal effects which may lead to: a reduction in renal function of the foetus, with possible oligohydramnios; neonatal renal insufficiency with hypotension and increased levels of potassium and even anuria (reversible or not).
As a consequence, the risk of malformation, if such a risk exists, is probably low. Termination of pregnancy does not appear to be appropriate if pregnancy occurs during treatment. However, the skull should be monitored by ultrasound.
In contrast, patients who discover they are pregnant while being treated with angiotensin-converting enzyme inhibitors must stop treatment immediately and for the duration of the pregnancy.
Lactation: In the absence of data, perindopril is contraindicated in women who are breastfeeding.
Linked to Indapamide: Pregnancy: As a general rule, the administration of diuretics should be avoided in pregnant women and should never be given as treatment for physiological oedema (and therefore do not require treatment) of pregnancy. Diuretics may lead to foeto-placental ischaemia, with a risk of impaired foetal growth.
Nonetheless, diuretics remain essential part of treatment of oedema from cardiac, hepatic and renal origin raised in pregnant women.
Lactation: Indapamide is excreted in small quantities in breast milk. Nonetheless, it should not be used in breastfeeding period due to the decrease and even suppression of the milk secretion; its undesirable effects in particular biological (potassium level); its belonging to sulphonamides with risks of allergy and nuclear icterus.
Use in children: The efficacy and tolerability of perindopril in children, alone or in combination, have not been established.
Use in the elderly: Renal function and potassium levels are tested before the start of treatment. The initial dose is subsequently adjusted according to blood pressure response, especially in cases of salt and water depletion, in order to avoid sudden onset of hypotension.



 Sign Out
Sign Out