


 Sign Out
Sign Out



Haemorrhagic risk: As with all anticoagulants, PRADAXA should be used with caution in conditions with an increased risk of bleeding. Bleeding can occur at any site during therapy with PRADAXA. An unexplained fall in hemoglobin and/or hematocrit or blood pressure should lead to a search for a bleeding site.
For situation of life-threatening or uncontrolled bleeding, when rapid reversal of the anticoagulation effects of dabigatran is required, the specific reversal agent (PRAXBIND, idarucizumab) is available (see "Surgery and Interventions, and Pre-operative Phase under Precautions" and "Overdosage".)
PRADAXA treatment does not require anticoagulant monitoring. The INR test is unreliable in patients on PRADAXA and false positive INR elevations have been reported. Therefore INR tests should not be performed.
Tests of anticoagulant activity such as thrombin time (TT), ecarin clotting time (ECT) and activated partial thromboplastin time (aPTT) are available to detect excessive dabigatran activity.
Dabigatran related anticoagulation can be assessed by ECT or TT. If ECT or TT is not available, the aPTT test provides an approximation of PRADAXA's anticoagulant activity.
Table 12 shows coagulation test thresholds at trough that may be associated with an increased risk of bleeding. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePrevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: In atrial fibrillation patients in RE-LY treated with 150 mg bid an aPTT of greater than 2.0 - 3.0 fold of normal range at trough was associated with an increased risk of bleeding.
Close clinical surveillance (looking for signs of bleeding or anaemia) is recommended throughout the treatment period, especially in the following situations that may increase the hemorrhagic risk: diseases associated with an increased risk of bleeding, such as congenital or acquired coagulation disorders, thrombocytopenia or functional platelet defects, active ulcerative gastrointestinal disease, recent biopsy or major trauma, recent intracranial haemorrhage or brain, spinal or ophthalmic surgery, bacterial endocarditis.
Pharmacokinetic studies demonstrated an increase in drug exposure in patients with reduced renal function including age-related decline of renal function. PRADAXA is contraindicated in cases of severe renal impairment (CrCL < 30 mL/min).
Patients who develop acute renal failure should discontinue PRADAXA.
Factors, such as decreased renal function (30 - 50mL/min CrCL), age ≥ 75 years, or strong P-gp-inhibitor comedication are associated with increased dabigatran plasma levels. The presence of one or more than one of these factors may increase the risk of bleeding (see "Dosage & Administration").
The concomitant use of PRADAXA with the following treatments has not been studied and may increase the risk of bleeding: unfractionated heparins (except at doses necessary to maintain patency of central venous or arterial catheter) and heparin derivatives, low molecular weight heparins (LMWH), fondaparinux, desirudin, thrombolytic agents, GPIIb/IIIa receptor antagonists, ticlopidine, dextran, sulfinpyrazone, rivaroxaban, prasugrel, vitamin K antagonists, and the P-gp inhibitors, itraconazole, tacrolimus, cyclosporine, ritonavir, tipranavir, nelfinavir and saquinavir.
The concomitant use of dronedarone increases exposure of dabigatran and is not recommended (see "Pharmacology: Pharmacokinetics: Special populations under Actions").
The concomitant use of ticagrelor increases the exposure to dabigatran and may show pharmacodynamic interaction, which may result in an increased risk of bleeding.
Bleeding risk may be increased in patients concomitantly treated with selective serotonin re-uptake inhibitors (SSRI) or selective serotonin norepinephrine re-uptake inhibitors (SNRIs).
Use of fibrinolytic agents for the treatment of acute ischemic stroke: The use of fibrinolytic agents for the treatment of acute ischemic stroke may be considered if the patient presents with a thrombin time (TT), or Ecarin clotting time (ECT), or activated partial thromboplastin time (aPTT) not exceeding the upper limit of normal (ULN) according to the local reference range.
In situations where there is an increased haemorrhagic risk (e.g. recent biopsy or major trauma, bacterial endocarditis) close observation (looking for signs of bleeding or anaemia) is generally required.
Primary prevention of venous thromboembolic events in adult patients who have undergone elective total hip replacement surgery or total knee replacement surgery: NSAIDs given for short-term perioperative analgesia have been shown not to be associated with increased bleeding risk when given in conjunction with PRADAXA. There is limited evidence regarding the use of regular NSAID medication with half-lives of less than 12 hours during treatment with PRADAXA and this has not suggested additional bleeding risk.
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: Co-administration of anti-platelet (including ASA and clopidogrel) and NSAID therapies increase the risk of bleeding. Specifically, with concomitant intake of antiplatelets or strong P-gp inhibitors in patients aged ≥75years, the risk of major bleeding, including gastrointestinal bleeding, increases. If bleeding is clinically suspected, appropriate measures such as testing for occult blood in stool, or testing for a drop in hemoglobin is suggested.
Interaction with P-gp inducers: The concomitant use of PRADAXA with the strong P-gp inducer rifampicin reduces dabigatran plasma concentrations. Other P-gp inducers such as St. John`s Wort or carbamazepine are also expected to reduce dabigatran plasma concentrations, and should be co-administered with caution (see "Interactions" and "Pharmacology: Pharmacokinetics: Special populations under Actions").
Surgery and Interventions: Patients on PRADAXA who undergo surgery or invasive procedures are at increased risk for bleeding. Therefore surgical interventions may require the temporary discontinuation of PRADAXA (see also "Pharmacology: Pharmacokinetics under Actions").
Patients can stay on PRADAXA while being cardioverted. PRADAXA treatment (150 mg twice daily) does not need to be interrupted in patients undergoing catheter ablation for atrial fibrillation (see "Dosage & Administration").
In case of emergency surgery or urgent procedures when rapid reversal of the anticoagulation effect is required the specific reversal agent (PRAXBIND, idarucizumab) to PRADAXA is available.
Reversing dabigatran therapy exposes patients to the thrombotic risk of their underlying disease. PRADAXA treatment can be re-initiated 24 hours after administration of PRAXBIND (idarucizumab), if the patient is clinically stable and adequate hemostasis has been achieved.
Preoperative Phase: Due to an increased risk of bleeding PRADAXA may be stopped temporarily in advance of invasive or surgical procedures.
Emergency Surgery or Urgent Procedure: The specific reversal agent (PRAXBIND, idarucizumab) of PRADAXA is available for the rapid reversal of the anticoagulation effect (see "Surgery and Interventions" as previously mentioned).
Acute Surgery/Intervention: If an acute intervention is required, PRADAXA should be temporarily discontinued. An acute surgery/intervention should be delayed if possible until at least 12 hours after the last dose. If surgery cannot be delayed there may be an increase in the risk of bleeding.
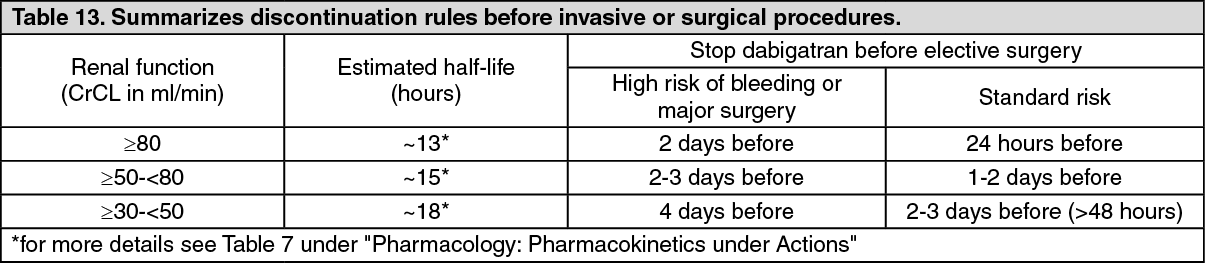
Elective Surgery/Intervention: If possible, PRADAXA should be discontinued at least 24 hours before invasive or surgical procedures. In patients at higher risk of bleeding or in major surgery where complete hemostasis may be required consider stopping PRADAXA 2-4 days before surgery. Clearance of dabigatran in patients with renal insufficiency may take longer. This should be considered in advance of any procedures (see Table 13 and also "Pharmacology: Pharmacokinetics under Actions"). (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePRADAXA is contraindicated in patients with severe renal dysfunction (CrCl <30 mL/min) but should this occur then PRADAXA should be stopped at least 5 days before major surgery.
If an acute intervention is required, PRADAXA should be temporarily discontinued. A surgery / intervention should be delayed if possible until at least 12 hours after the last dose. If surgery cannot be delayed there may be an increase in the risk of bleeding. This risk of bleeding should be weighed together with the urgency of intervention.
Patients with moderate renal impairment have an increased exposure to dabigatran. Limited data is available in patients < 50 kg and the elderly. In these situations, PRADAXA should be used with caution and a close clinical surveillance (looking for signs of bleeding or anemia) is required throughout the treatment period. When severe bleedings occur treatment must be discontinued and the source of bleeding investigated. Agents that may enhance the risk of haemorrhage should not be administered concomitantly or should be administered with caution with PRADAXA.
Patients at high surgical mortality risk and with intrinsic risk factors for thromboembolic events: There are limited efficacy and safety data for dabigatran available in these patients and therefore they should be treated with caution.
Spinal anesthesia/epidural anesthesia/lumbar puncture: Procedures such as spinal anesthesia may require complete hemostatic function. The risk of spinal or epidural haematoma may be increased in cases of traumatic or repeated puncture and by the prolonged use of epidural catheters. After removal of a catheter, an interval of at least 2 hours should elapse before the administration of the first dose of PRADAXA. These patients require frequent observation for neurological signs and symptoms of spinal or epidural hematoma.
Post Procedural Period: Resume treatment after complete haemostasis is achieved.
Hip fracture surgery: There is no data on the use of PRADAXA in patients undergoing hip fracture surgery. Therefore treatment is not recommended.
Myocardial Infarction (DVT/PE): In the three active controlled studies, a higher rate of MI was reported in patients who received dabigatran etexilate than in those who received warfarin: 0.4% vs. 0.2% in the short-term RE-COVER and RE-COVER II studies; and 0.8% vs. 0.1% in the long-term RE-MEDY trial. The increase was statistically significant in this study (p=0.022).
In the RE-SONATE study, which compared dabigatran etexilate to placebo, the rate of MI was 0.1% for patients who received dabigatran etexilate and 0.2% for patients who received placebo.
Active Cancer Patients (DVT/PE): The efficacy and safety have not been established for DVT/PE patients with active cancer.
Effects on ability to drive and use machines: No studies on the effects on the ability to drive and use machines have been performed.