


 Sign Out
Sign Out



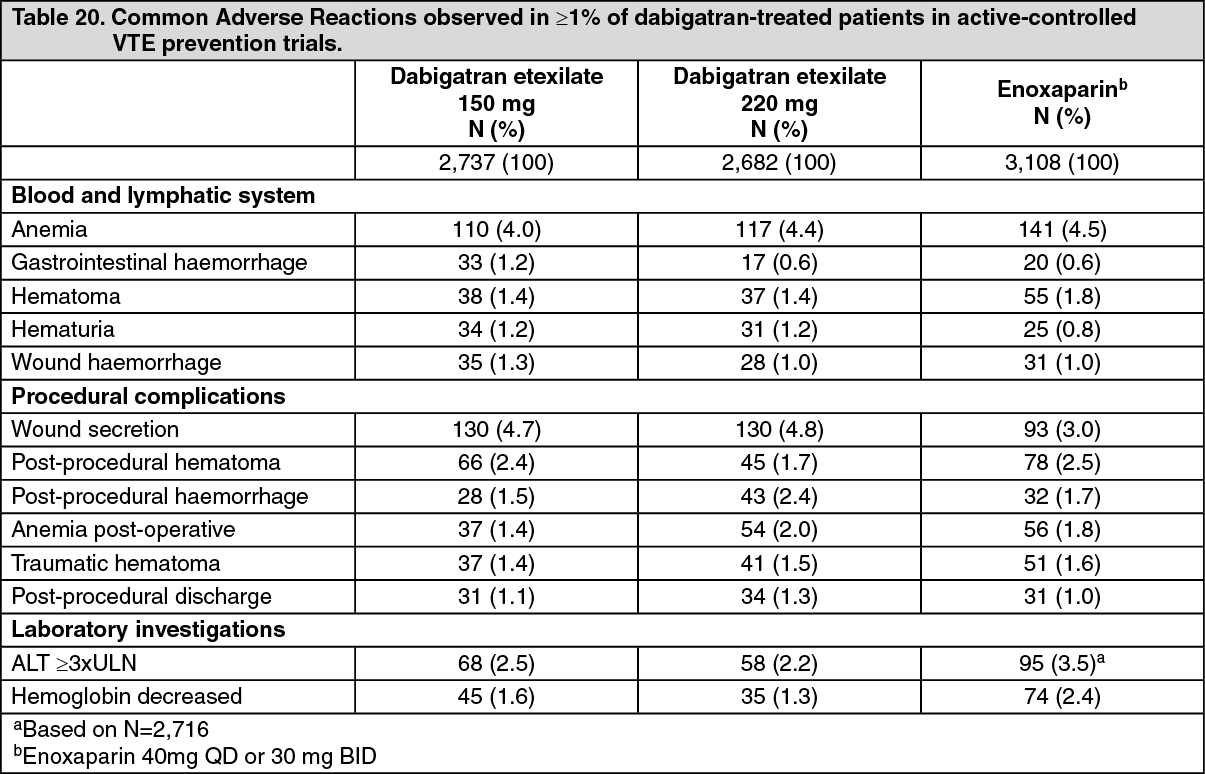
Primary prevention of venous thromboembolic events in adult patients who have undergone elective total hip replacement surgery or total knee replacement surgery: In the primary VTE prevention trials after elective total hip replacement or total knee replacement surgery, a total of 10,795 patients were treated in 6 controlled studies with at least one dose of dabigatran etexilate (150mg qd, 220mg qd, enoxaparin). 6,684 of the 10,795 patients were treated with 150 mg or 220 mg once daily of dabigatran etexilate. In total, about 9% of patients treated with dabigatran and about 10% of patients treated with enoxaparin for VTE prevention after elective hip or knee surgery (short-term treatment up to 42 days) experienced adverse reactions.
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: In the RELY trial investigating the prevention of stroke and systemic embolism in patients with atrial fibrillation, a total of 12,042 patients were treated with dabigatran etexilate. Of these 6,059 were treated with 150 mg twice daily of dabigatran etexilate, while 5,983 received doses of 110 mg twice daily.
About 22% of patients with atrial fibrillation treated with dabigatran and about 16% of patients treated with warfarin for the prevention of stroke and systemic embolism (long-term treatment for up to 3 years) experienced adverse events considered related to treatment.
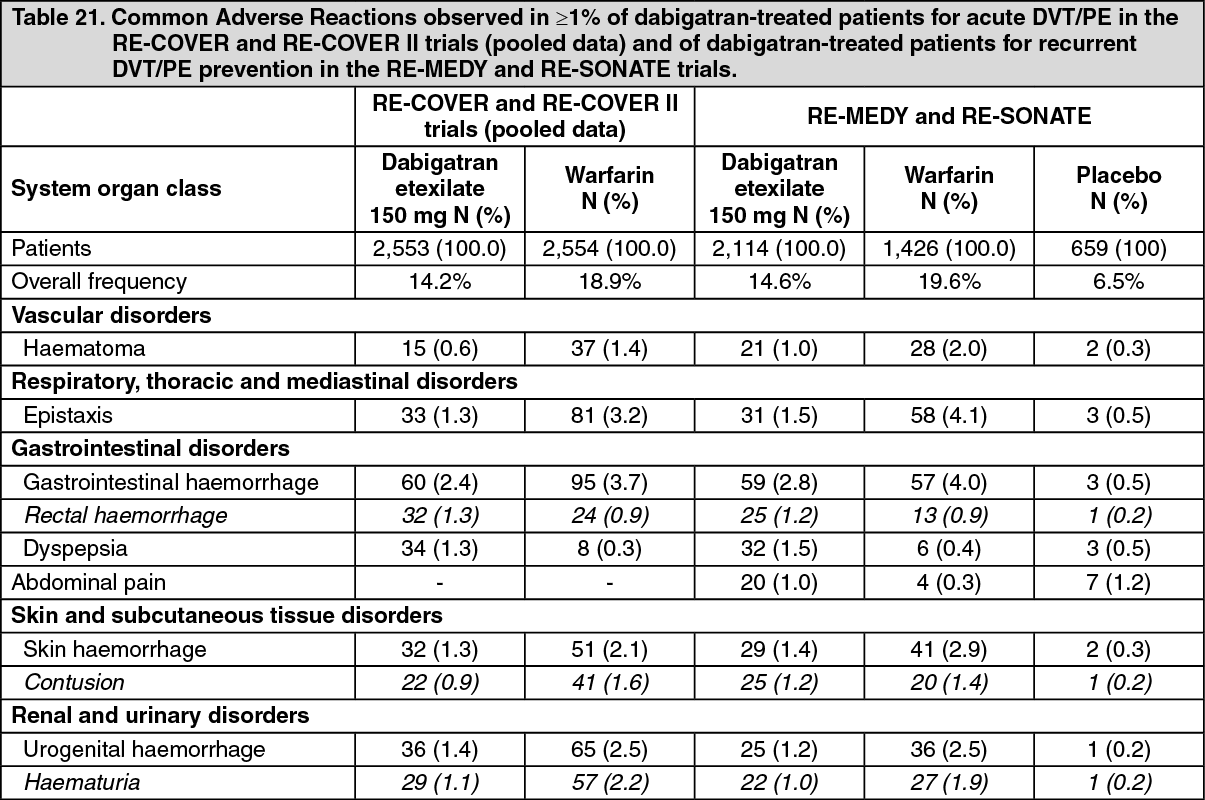
Treatment of acute deep vein thrombosis (DVT) and/or pulmonary embolism (PE): In the acute DVT/PE treatment trials (RE-COVER, RE-COVER II) a total of 2,553 patients were included in the safety analysis for dabigatran etexilate. All patients were treated with dabigatran etexilate 150 mg bid. 14% of patients treated for acute DVT/PE treatment (long-term treatment up to 6 months) experienced adverse reactions.
Prevention of recurrent deep vein thrombosis (DVT) and/or pulmonary embolism (PE): In the recurrent DVT/PE prevention trials (RE-MEDY, RE-SONATE) a total of 2,114 patients were treated with dabigatran etexilate; 552 of the 2,114 patients were rolled over from the RE-COVER trial (acute DVT/PE treatment) into the RE-MEDY trial and are counted in both the acute and recurrent patient totals. All patients were treated with dabigatran etexilate 150 mg bid and 15% of patients treated for recurrent DVT/PE prevention (long-term treatment up to 36 months) experienced adverse reactions.
Bleeding: Bleeding is the most relevant side effect of PRADAXA. Bleeding of any type or severity occurred in approximately 14 % of patients treated short-term for elective hip or knee replacement surgery; in long-term treatment in 16.6 % of patients with atrial fibrillation treated long-term for the prevention of stroke and systemic embolism; and in 14.4% of patients with acute DVT and/or PE. In the recurrent DVT/PE trial RE-MEDY 19.4% and in the RE-SONATE trial 10.5% of patients experienced any bleeding.
Although rare in frequency in clinical trials, major or severe bleeding may occur and, regardless of location, may lead to disabling, life-threatening or even fatal outcomes.
Since the patient populations treated with PRADAXA for different indications are not interchangeable, a summary description of major and total bleeding is provided by indication and/or trial in Tables 14, 15 and 16 as follows.
Prevention of VTE after THR or TKR surgery: See Tables 14 and 15.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image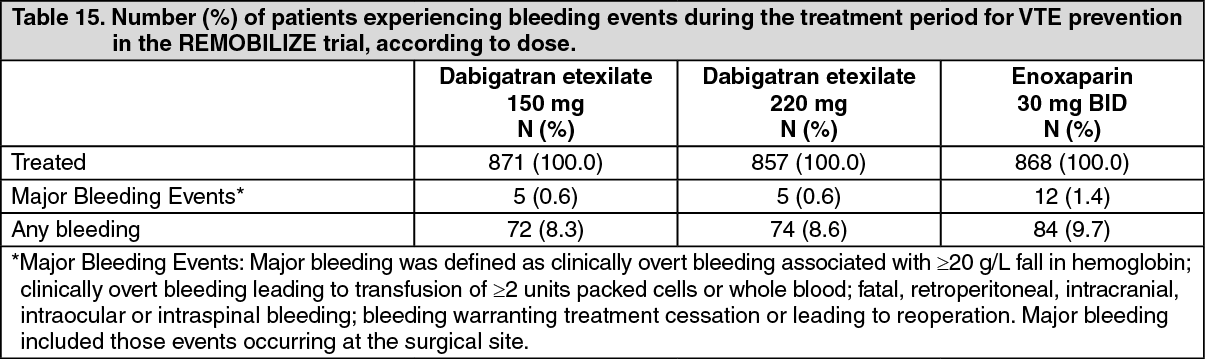 Click on icon to see table/diagram/image
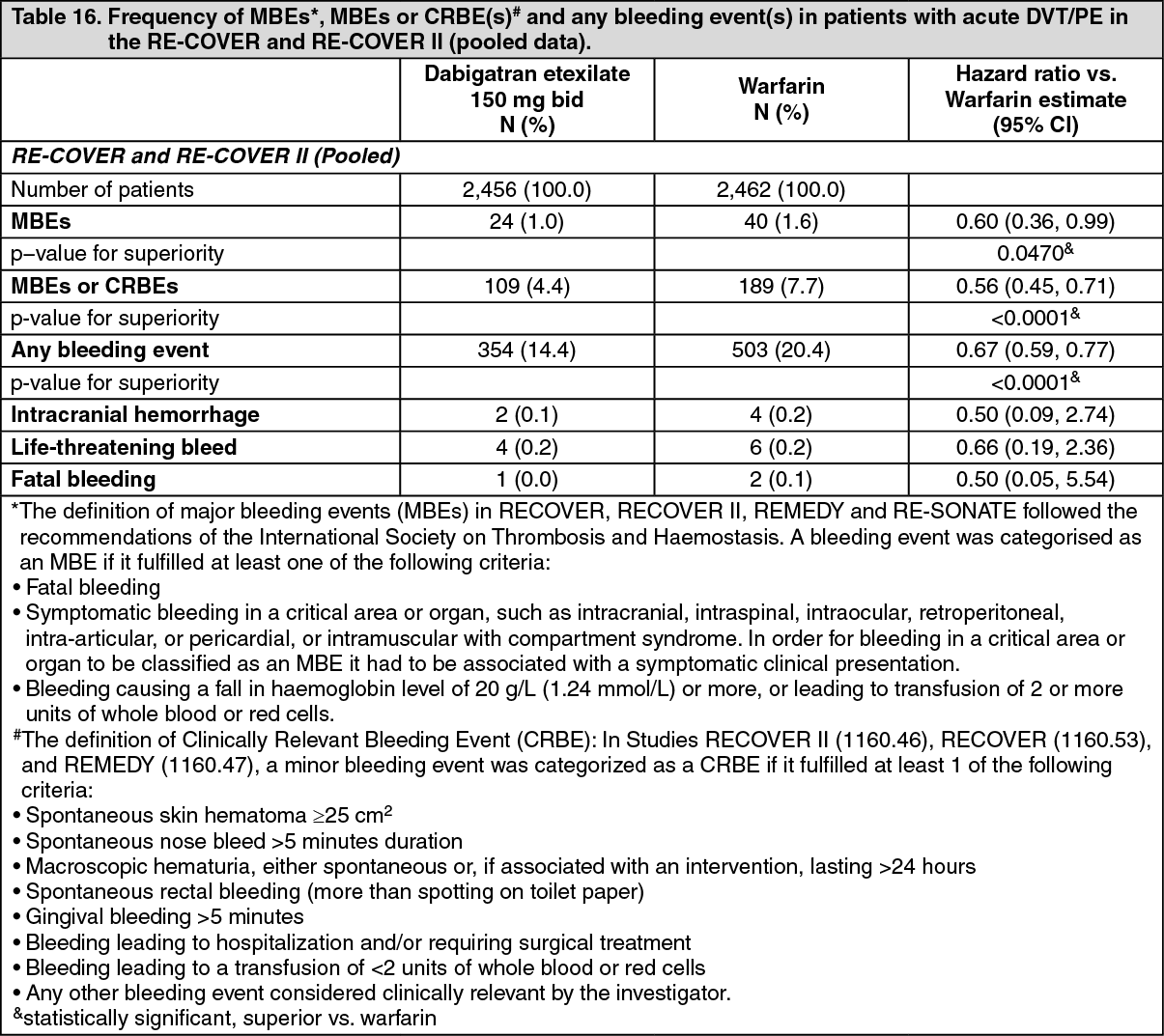
Click on icon to see table/diagram/imageTreatment of VTE and Prevention of Recurrent DVT and PE: See Table 16.
 Click on icon to see table/diagram/image
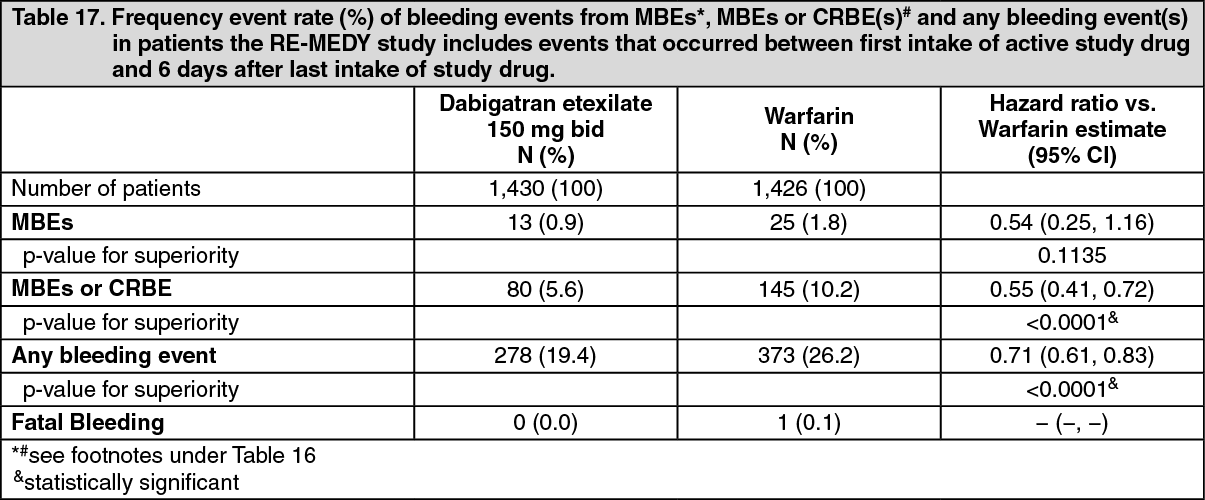
Click on icon to see table/diagram/imageBleeding events for both treatments are counted from the first intake of dabigatran etexilate or warfarin after the parenteral therapy has been discontinued (oral only treatment period). This includes all bleeding events which occurred during dabigatran therapy. All bleeding events which occurred during warfarin therapy are included except for those during the overlap period between warfarin and parenteral therapy. (See Tables 17 and 18.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image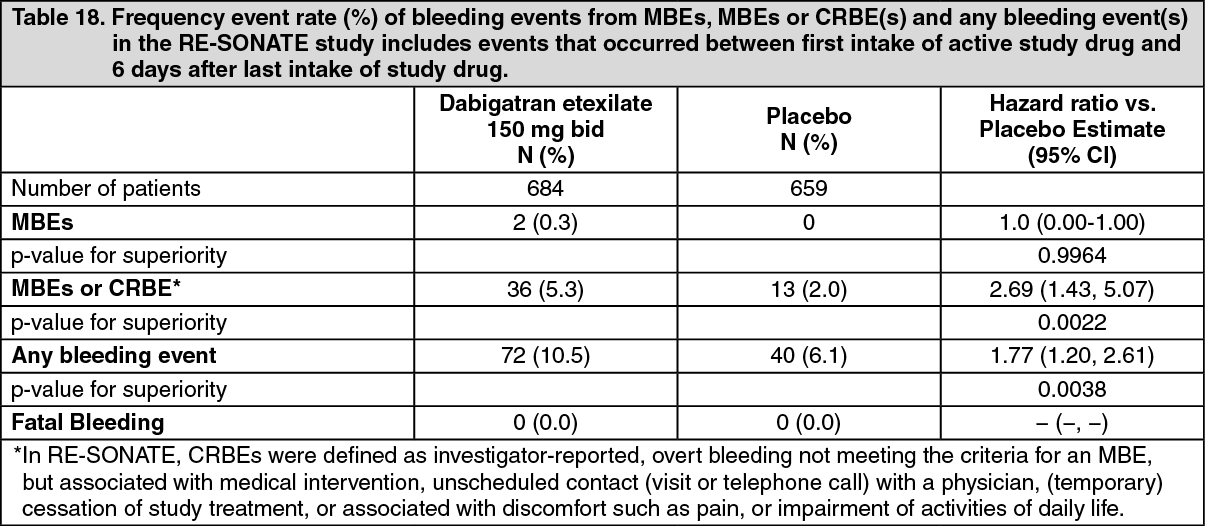 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePrevention of stroke and systemic embolism in AF patients - the RELY trial: In Table 19, the category of major bleeds includes both life-threatening and non-life threatening bleeds. Intracranial bleeds is a subcategory of life-threatening bleeds. Intracranial bleeds include intracerebral (haemorrhagic stroke), subarachnoid and subdural bleeds. For this reason, these events may be counted in multiple categories. (See Table 19.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePrevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: Major bleeding fulfilled one or more of the following criteria: Bleeding associated with a reduction in hemoglobin of at least 20 grams per litre or leading to a transfusion of at least 2 units of blood or packed cells; Symptomatic bleeding in a critical area or organ: intraocular, intracranial, intraspinal or intramuscular with compartment syndrome, retroperitoneal bleeding, intra-articular bleeding or pericardial bleeding.
Major bleeds were classified as life-threatening if they fulfilled one or more of the following criteria: Fatal bleed; symptomatic intracranial bleed; reduction in hemoglobin of at least 50 grams per litre; transfusion of at least 4 units of blood or packed cells; a bleed associated with hypotension requiring the use of intravenous inotropic agents; a bleed that necessitated surgical intervention.
Subjects randomized to dabigatran etexilate 110 mg twice daily and 150mg twice daily had a significantly lower risk for life-threatening bleeds, haemorrhagic stroke and intracranial bleeding compared to warfarin [p< 0.05]. Both dose strengths of dabigatran etexilate had also a statistically significant lower total bleed rate. Subjects randomized to dabigatran etexilate 110mg twice daily had a significantly lower risk for major bleeds compared with warfarin (hazard ratio 0.81, p=0.0027).
Treatment of acute deep vein thrombosis (DVT) and/or pulmonary embolism (PE): The definition of major bleeding events (MBEs) followed the recommendations of the International Society on Thrombosis and Haemostasis. A bleeding event was categorised as an MBE if it fulfilled at least one of the following criteria: Fatal bleeding; Symptomatic bleeding in a critical area or organ, such as intracranial, intraspinal, intraocular, retroperitoneal, intra-articular, or pericardial, or intramuscular with compartment syndrome. In order for bleeding in a critical area or organ to be classified as an MBE it had to be associated with asymptomatic clinical presentation; Bleeding causing a fall in haemoglobin level of 20 g/L (1.24 mmol/L) or more, or leading to transfusion of 2 or more units of whole blood or red cells.
In a pooled analysis of the two pivotal trials (RE-COVER, RE-COVER II) in acute DVT/PE treatment, subjects randomized to dabigatran etexilate had lower rates of the following bleeding events, which were statistically significant: Major bleeding events (hazard ratio 0.60 (0.36, 0.99)); Major or clinically relevant bleeding events (CRBEs) (hazard ratio 0.56 (0.45, 0.71)); Any bleeding events (hazard ratio 0.67 (0.59, 0.77)).
All of which were superior vs. warfarin.
Bleeding events for both treatments are counted from the first intake of dabigatran etexilate or warfarin after the parenteral therapy has been discontinued (oral only treatment period). This includes all bleeding events which occurred during dabigatran therapy. All bleeding events which occurred during warfarin therapy are included except for those during the overlap period between warfarin and parenteral therapy.
Prevention of recurrent deep vein thrombosis (DVT) and/or pulmonary embolism (PE): The definition of MBEs followed the recommendations of the International Society on Thrombosis and Haemostasis. A bleeding in RE-MEDY event was categorised as an MBE if it fulfilled at least one of the following criteria: Fatal bleeding; Symptomatic bleeding in a critical area or organ, such as intracranial, intraspinal, intraocular, retroperitoneal, intra-articular, or pericardial, or intramuscular with compartment syndrome. In order for bleeding in a critical area or organ to be classified as an MBE it had to be associated with asymptomatic clinical presentation; Bleeding causing a fall in haemoglobin level of 20 g/L (1.24 mmol/L) or more, or leading to transfusion of 2 or more units of whole blood or red cells.
In RE-MEDY, patients randomized to dabigatran etexilate had significantly less bleeds compared to warfarin for the following categories: major bleeding events or clinically relevant bleeding events (hazard ratio 0.55 (0.41, 0.72), p<0.0001) and any bleeding events (hazard ratio 0.71 (0.61, 0.83), p<0.0001).
A bleeding event in RE-SONATE was categorised as an MBE if it fulfilled at least one of the following criteria: Fatal bleeding; Associated with a fall in haemoglobin of 2 g/dL or more; Led to the transfusion of ≥2 units packed cells or whole blood; Occurred in a critical site: intracranial, intraspinal, intraocular, pericardial, intra-articular, intramuscular with compartment syndrome, retroperitoneal.
In RE-SONATE, the rates of MBE were low (2 patients with MBEs (0.3%) for dabigatran etexilate vs. 0 patients with MBE (0%) for placebo. The rate of major bleeding events or clinically relevant bleeding events were higher with dabigatran etexilate compared with placebo (5.3% vs. 2.0%).
Clinical Trial Adverse Drug Reactions: Because clinical trials are conducted under very specific conditions the adverse reaction rates observed in the clinical trials may not reflect the rates observed in practice and should not be compared to the rates in the clinical trials of another drug. Adverse drug reaction information from clinical trials is useful for identifying drug-related adverse events and for approximating rates.
Prevention of VTE after THR or TKR surgery: See Table 20.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTreatment of VTE and Prevention of Recurrent DVT and PE: See Table 21.
 Click on icon to see table/diagram/image
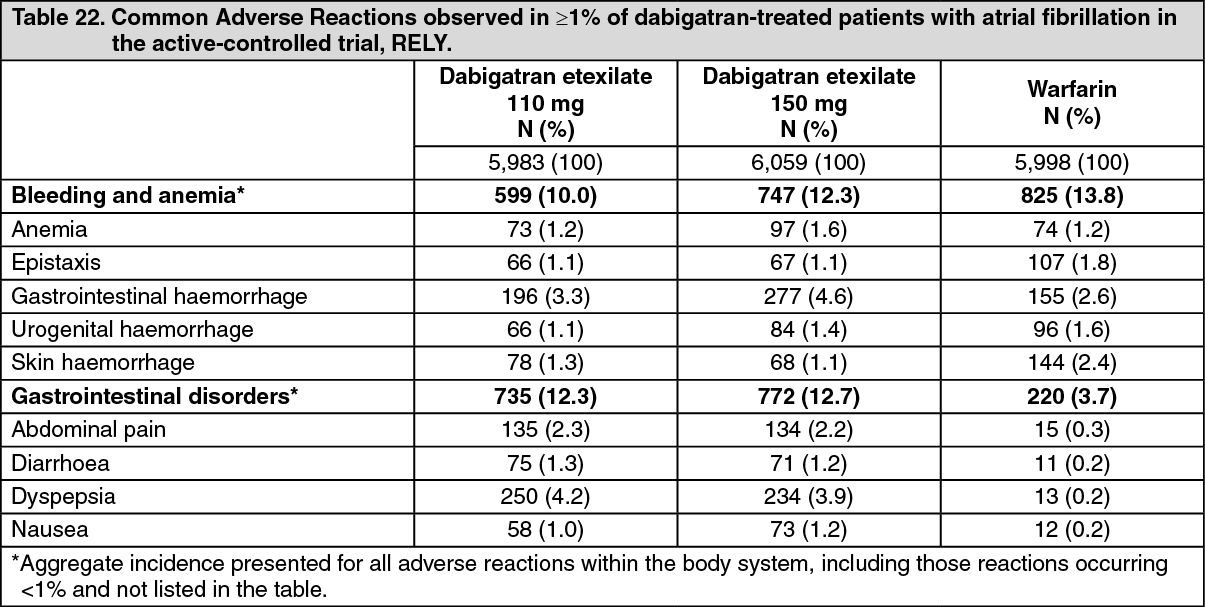
Click on icon to see table/diagram/imagePrevention of stroke and systemic embolism in AF patients - RELY trial: See Table 22.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageGastrointestinal adverse reactions occurred more often with dabigatran etexilate than warfarin. These were related to dyspepsia (including upper abdominal pain, abdominal pain, abdominal discomfort, epigastric discomfort), or gastritis-like symptoms (including GERD, esophagitis, erosive gastritis, gastric haemorrhage, hemorrhagic gastritis, hemorrhagic erosive gastritis, gastrointestinal ulcer).
Gastrointestinal (GI) haemorrhage occurred at a higher frequency with PRADAXA 150 mg bid, compared to warfarin (see Table 22 as previously mentioned). GI adjudicated major bleeds were reported at 1.1, 1.6%, and 1.1% (annualized rates) in the DE 110 mg, DE 150 mg and warfarin groups, respectively. GI life-threatening bleeds occurred with a frequency of 0.6%, 0.8% and 0.5% in the DE 110 mg, DE 150 mg and warfarin groups, respectively. Any GI bleeds occurred with frequency of 5.4%, 5.7% and 3.9% in the DE 110 mg, DE 150 mg and warfarin groups, respectively. The underlying mechanism of the increased rate of GI bleeding has not been established (see Pharmacology: Clinical trials in prevention of stoke and systemic embolism in patients with atrial fibrillation under Actions).
Allergic reactions or drug hypersensitivity including angioedema, urticaria, bronchospasm, rash and pruritus have been reported in patients who received dabigatran etexilate. Rare cases of anaphylactic reactions have also been reported.
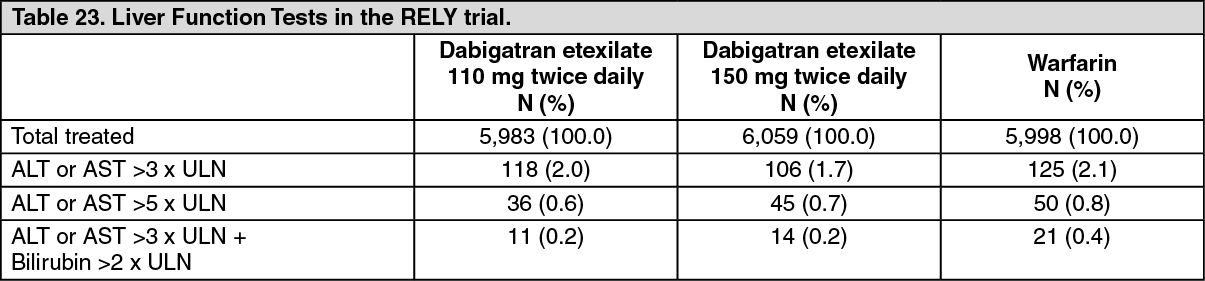
Liver Function Tests: In the long-term RELY study, observed abnormalities of liver function tests (LFT) are presented as follows in Table 23. (See Table 23.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the active controlled studies RE-COVER, RE-COVER II and RE-MEDY, potential abnormalities of LFTs occurred with a comparable or lower incidence in dabigatran etexilate vs. warfarin treated patients. In RE-SONATE, there was no marked difference between the dabigatran- and placebo groups with regard to possible clinically significant abnormal LFT values.
Less Common Clinical Trial Adverse Drug Reactions (<1%): Prevention of VTE after THR or TKR surgery (dabigatran 150 mg and 220 mg/day): Blood and lymphatic system: thrombocytopenia.
Gastrointestinal disorders: hemorrhoidal haemorrhage, rectal haemorrhage.
General: bloody discharge, catheter site haemorrhage.
Hepatobiliary disorders: alanine aminotransferase increased, aspartate aminotransferase increased, hepatic enzyme increased, hepatic function abnormal/liver function test abnormal, transaminases increased.
Injury, poisoning and procedural complications: incision site haemorrhage.
Laboratory Investigations: occult blood positive, blood urine present, hematocrit decrease.
Musculoskeletal and cumulative tissue disorders: hemarthrosis.
Respiratory and thoracic system: epistaxis.
Skin and sub-cutaneous tissue: ecchymosis.
Surgical and medical procedures: post-procedural drainage, wound drainage.
Vascular disorders: haemorrhage.
Treatment of VTE and Prevention of Recurrent DVT and PE (dabigatran 150 mg bid): Blood and lymphatic system disorders: anaemia, thrombocytopenia.
Vascular disorders: haematoma, haemorrhage.
Gastrointestinal disorders: diarrhoea, dysphagia, gastrointestinal ulcer (including esophageal ulcer), gastro-esophagitis, gastro-esophageal reflux disease, nausea, vomiting.
Hepatobiliary disorders: hepatic function abnormal.
Musculoskeletal and connective tissue and bone disorders: hemarthrosis.
General disorders and administration site conditions: catheter site haemorrhage, injection site haemorrhage.
Injury, poisoning and procedural complications: incision site haemorrhage, traumatic haemorrhage.
Immune system disorder: anaphylaxis*, angioedema, drug hypersensitivity (bronchospasm*, pruritus, rash, urticaria).
Respiratory disorders: hemoptysis.
Nervous system disorders: intracranial haemorrhage.
* These side effects were not reported in clinical trials as ADRs (AEs only); therefore, a frequency could not be calculated.
Prevention of stroke and systemic embolism in AF patients - the RE-LY trial (dabigatran 110 mg bid and 150 mg bid): Blood and lymphatic system disorders: thrombocytopenia.
Vascular disorders: haematoma, haemorrhage.
Gastrointestinal disorders: gastrointestinal ulcer (including oesophageal ulcer), gastro-esophagitis, gastro-esophageal reflux disease, vomiting, dysphagia.
Hepatobiliary disorders: hepatic function abnormal / liver function test abnormal, hepatic enzyme increased.
Musculoskeletal and connective tissue and bone disorders: haemarthrosis.
Renal and urinary disorders: urogenital haemorrhage.
General disorders and administration site conditions: injection site haemorrhage, catheter site haemorrhage.
Injury, poisoning and procedural complications: incision site haematoma, incision site haemorrhage, traumatic haemorrhage, traumatic hematoma.
Immune system disorder: anaphylaxis, drug hypersensitivity (bronchospasm*, pruritus, rash, urticaria).
Respiratory disorders: haemoptysis.
Nervous system disorders: intracranial haemorrhage.
* These side effects were not reported in clinical trials as ADRs (AEs only).