


 Sign Out
Sign Out



Pharmacology: Dabigatran etexilate is a small molecule prodrug which does not exhibit any pharmacological activity. After oral administration, dabigatran etexilate is rapidly absorbed and converted to dabigatran by esterase-catalysed hydrolysis in plasma and in the liver. Dabigatran is a potent, competitive, reversible direct thrombin inhibitor and is the main active principle in plasma.
Since thrombin (serine protease) enables the conversion of fibrinogen into fibrin during the coagulation cascade, its inhibition prevents the development of thrombus. Dabigatran also inhibits free thrombin, fibrin-bound thrombin and thrombin-induced platelet aggregation.
In-vivo and ex-vivo animal studies have demonstrated antithrombotic efficacy and anticoagulant activity of dabigatran after intravenous administration and of dabigatran etexilate after oral administration in various animal models of thrombosis.
There is a close correlation between plasma dabigatran concentrations and degree of anticoagulant effect. Dabigatran prolongs the aPTT, ECT and TT.
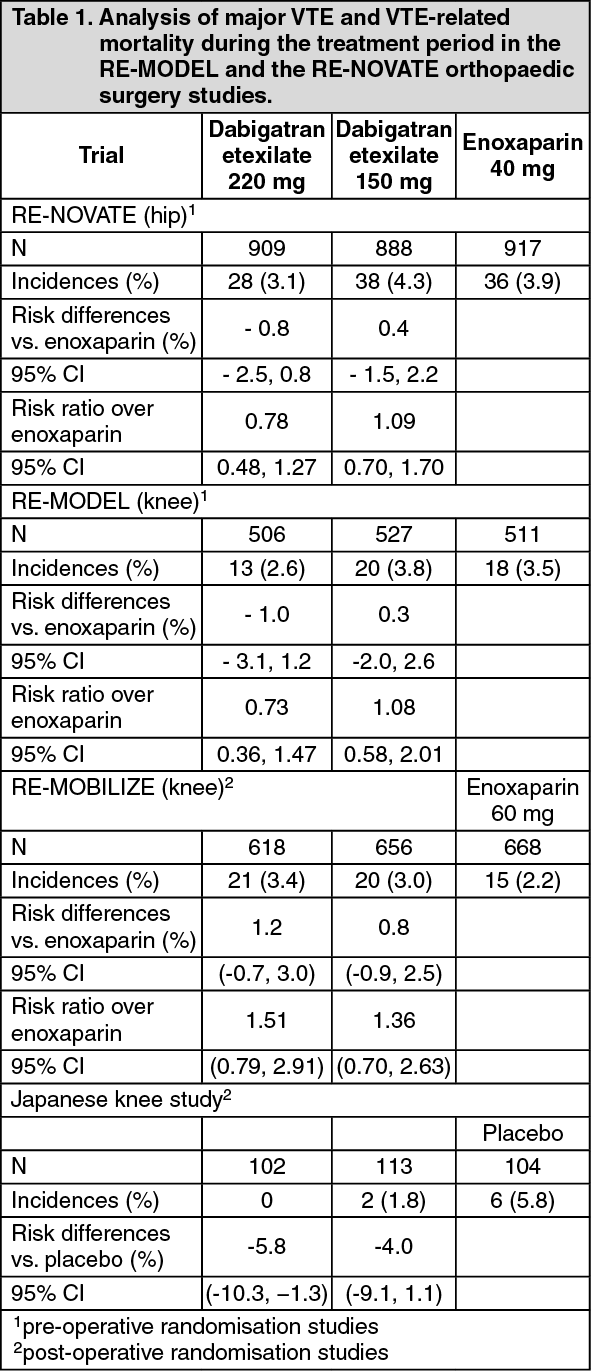
Clinical trials in primary VTE prevention following major joint replacement surgery: In 2 large randomized, parallel group, double-blind, dose-confirmatory trials, patients undergoing elective major orthopaedic surgery (one for knee replacement surgery and one for hip replacement surgery) received dabigatran etexilate 75 mg or 110 mg within 1-4 hours of surgery followed by 150 or 220 mg once daily thereafter, haemostasis having been secured, or enoxaparin 40 mg on the day prior to surgery and once daily thereafter.
In the RE-MODEL trial (knee replacement) treatment was for 6 - 10 days and in the RE-NOVATE trial (hip replacement) for 28 - 35 days. Totals of 2076 patients (knee) and 3494 (hip) were treated respectively.
The results of the knee study (RE-MODEL) with respect to the primary end-point, total including asymptomatic venous thromboembolism (VTE) plus all-cause mortality showed that the antithrombotic effect of both doses of dabigatran etexilate were statistically non-inferior to that of enoxaparin.
Similarly, total including asymptomatic VTE and all-cause mortality constituted the primary end-point for the hip study (RE-NOVATE). Again dabigatran etexilate at both once daily doses was statistically non-inferior to enoxaparin 40 mg daily.
Furthermore in a third randomized, parallel group, double-blind, trial (RE-MOBILIZE), patients undergoing elective total knee surgery received dabigatran etexilate 75 mg or 110 mg within 6-12 hours of surgery followed by 150 mg and 220 mg once daily thereafter. The treatment duration was 12-15 days. In total 2615 patients were randomised and 2596 were treated. The comparator dosage of enoxaparin was 30 mg twice daily according to the US label. In the RE-MOBILIZE trial non-inferiority was not established. There were no statistical differences in bleeding between the comparators.
In addition a randomized, parallel group, double-blind, placebo-controlled phase II study in Japanese patients where dabigatran etexilate 110 mg, 150 mg, and 220 mg was administered at the next day after elective total knee replacement surgery was evaluated. The Japanese study showed a clear dose response relationship for the efficacy of dabigatran etexilate and a placebo like bleeding profile.
In RE-MODEL and RE-NOVATE the randomisation to the respective study medication was done pre-surgery, and in the RE-MOBILIZE and the Japanese placebo controlled trial the randomisation to the respective study medication was done post-surgery. This is of note especially in the safety evaluation of these trials. For this reason the trials are grouped in pre- and post surgery randomised trials in Table 1.
Data for the major VTE and VTE-related mortality end-point and adjudicated major bleeding endpoints are shown in the Table 1 as follows. VTE was defined as the composite incidence of deep vein thrombosis and Pulmonary Embolism. (See Table 1.)
 Click on icon to see table/diagram/image
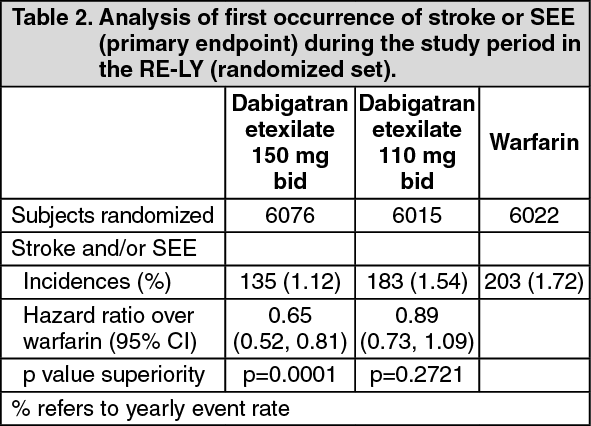
Click on icon to see table/diagram/imageClinical trials in prevention of stroke and systemic embolism in patients with atrial fibrillation: The clinical evidence for the efficacy of dabigatran etexilate is derived from the RE-LY study (Randomized Evaluation of Long term anticoagulant therapy) a multi-center, multi-national, randomized parallel group study of two blinded doses of dabigatran etexilate (110 mg bid and 150 mg bid) compared to open-label warfarin in patients with atrial fibrillation at moderate to high risk of stroke or systemic embolism. The primary objective in this study was to determine if dabigatran was non-inferior to warfarin in reducing the occurrence of the composite endpoint, stroke and systemic embolic events (SEE).
In the RE-LY study, a total of 18,113 patients were randomized, with a mean age of 71.5 years and a mean CHADS2 score of 2.1. The population had approximately equal proportions of patients with CHADS2 score 1, 2 and ≥3. The patient population was 64% male, 70% Caucasian and 16% Asian. RE-LY had a median treatment of 20 months with dabigatran etexilate given as fixed dose without coagulation monitoring. In addition to documented non-valvular atrial fibrillation (AF) e.g., persistent AF or paroxysmal, patients had one of the following additional risk factors for stroke: Previous stroke, transient ischemic attack, or systemic embolism; Left ventricular ejection fraction <40 %; Symptomatic heart failure, ≥ NYHA Class 2; Age ≥ 75 years; Age ≥ 65 years associated with one of the following: diabetes mellitus, coronary artery disease, or hypertension.
The concomitant diseases of patients in this trial included hypertension 79%, diabetes 23% and coronary artery disease (CAD) 28%. 50% of the patient population was VKA naïve defined as less than 2 months total life time exposure. 32% of the population had never been exposed to a VKA. For those patients randomized to warfarin, the time in therapeutic range (INR 2.0 to 3.0) for the trial was a median of 67%. Concomitant medications included ASA (25% of subjects used at least 50% of the time in study), clopidogrel (3.6%), ASA+clopidogrel (2%), NSAIDs (6.3%), beta-blockers (63.4%), diuretics (53.9%), statins (46.4%), ACE-inhibitors (44.6%), angiotensin receptor blockers (26.1%), oral hypoglycemics (17.5%), insulin (5.2%), digoxin (29.4%), amiodarone (11.3%), diltiazem (8.9%), verapamil (5.4%), and proton pump inhibitors (17.8%).
For the primary endpoint, stroke and systemic embolism, no subgroups (i.e., age, weight, gender, renal function, ethnicity, etc.) were identified with a different risk ratio compared to warfarin.
This study demonstrated that dabigatran etexilate, at a dose of 110 mg twice daily, is non-inferior to warfarin in the prevention of stroke and systemic embolism in subjects with atrial fibrillation, with a reduced risk of intracranial hemorrhage and total bleeding. The higher dose of 150 mg twice daily, reduces significantly the risk of ischemic and hemorrhagic stroke, vascular death, intracranial hemorrhage and total bleeding compared to warfarin. The lower dose of dabigatran has a significantly lower risk of major bleeding compared to warfarin.
Figure 1 and Tables 2 - 6 display details of key results. (See Table 2, Figure 1, and Tables 3 and 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image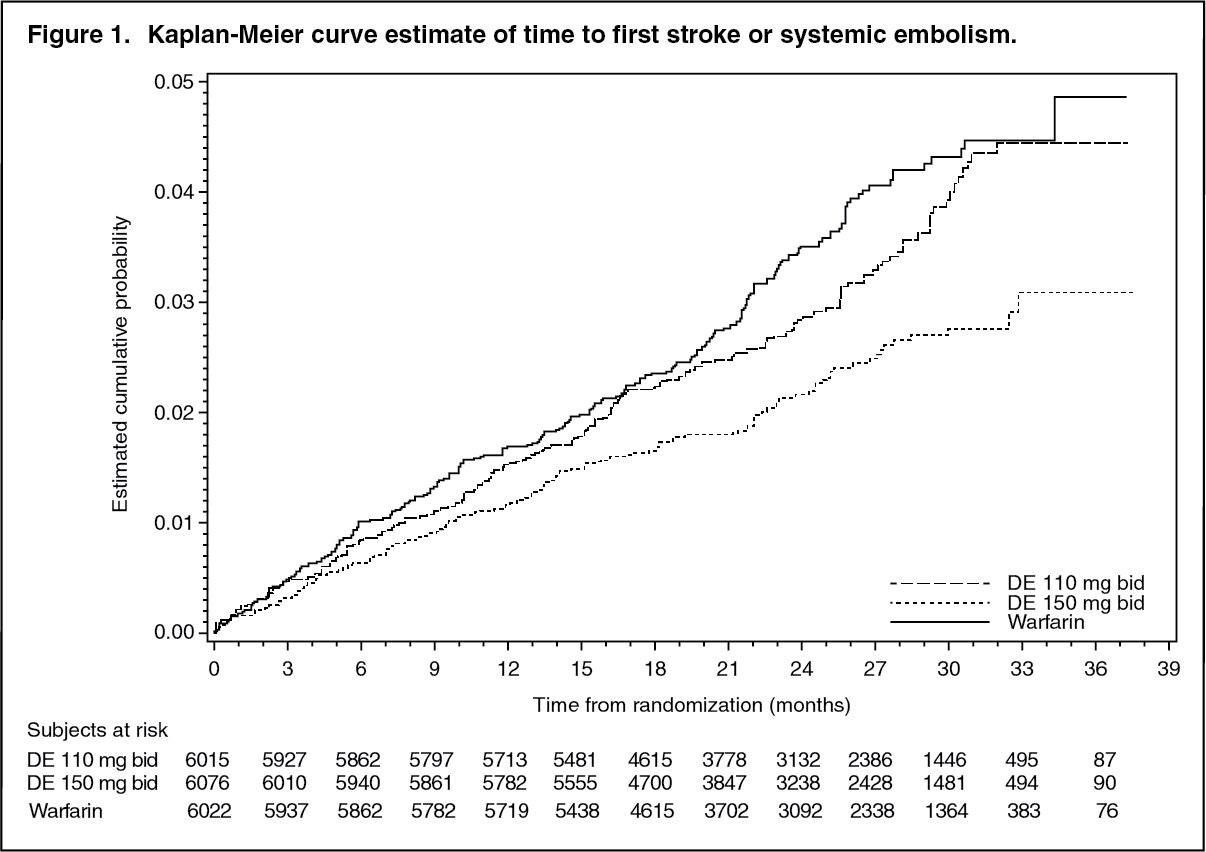 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image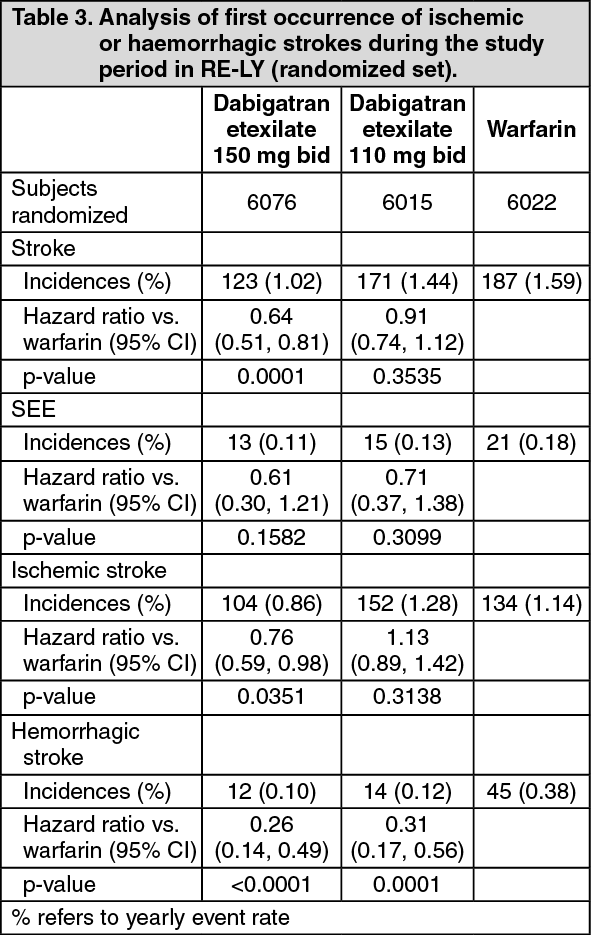 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image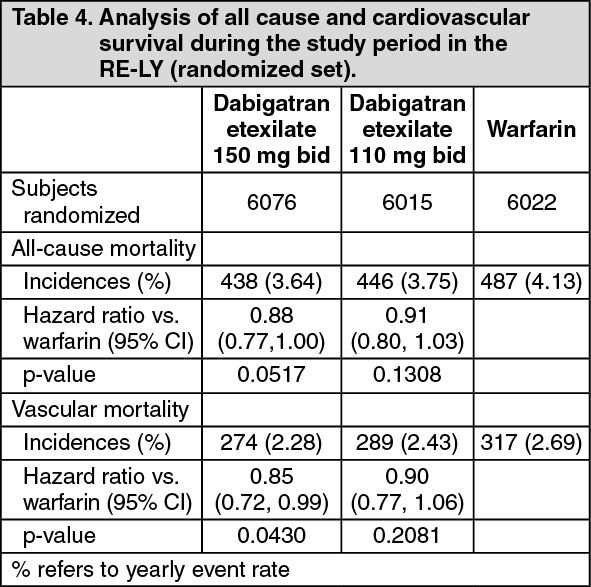 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe net clinical benefit (NCB) as measured by the unweighted composite clinical endpoint of stroke, systemic embolism, pulmonary embolism, acute myocardial infarction, vascular deaths, and major bleeds was assessed and is presented as part of Table 5. The yearly event rates for the dabigatran etexilate groups were lower compared to the warfarin group. The risk reduction for this composite endpoint was 8% and 10% for the dabigatran etexilate 110 mg bid and 150 mg bid treatment groups. (See Table 5.)
 Click on icon to see table/diagram/image
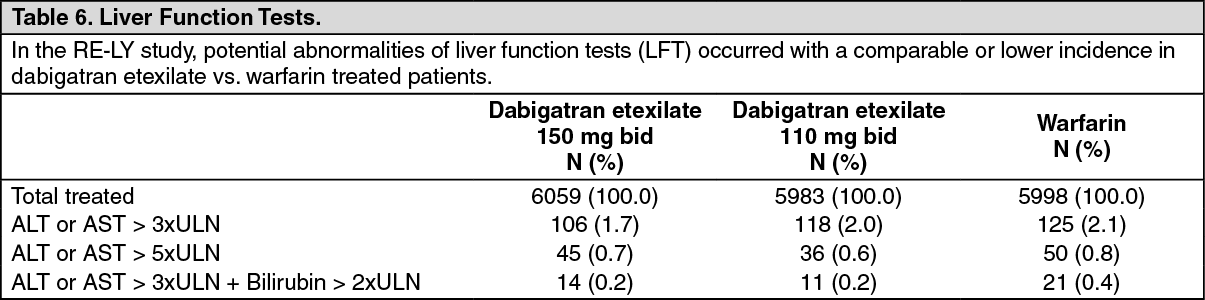
Click on icon to see table/diagram/imageThere was an increased numeric imbalance in MI events in subjects treated with dabigatran compared to warfarin treated subjects. The reason for this imbalance is unknown. Patients treated with dabigatran who have risk factors for coronary artery disease should be treated according to local guidelines. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe RE-LY extension study (RELY-ABLE) provided additional safety information for a large cohort of patients which continued the same dose of dabigatran etexilate as assigned in the RE-LY trial. Patients were eligible for the RELY-ABLE trial if they had not permanently discontinued study medication at the time of their final RE-LY study visit. Enrolled patients continued to receive the same double-blind dabigatran etexilate dose randomly allocated in RE-LY, for up to 43 months of follow up after RE-LY (total mean follow-up RE-LY + RELY-ABLE, 4.5 years). There were 5897 patients enrolled, representing 49% of patients originally randomly assigned to receive dabigatran etexilate in RE-LY and 86% of RELY-ABLE-eligible patients.
During the additional 2.5 years of treatment in RELY-ABLE, with a maximum exposure of over 6 years (total exposure in RELY + RELY-ABLE), the long-term safety profile of dabigatran etexilate was confirmed for both test doses. No new safety findings were observed.
The rates of outcome events including, major bleed and other bleeding events were consistent with those seen in RE-LY.
Patients undergoing catheter ablation for atrial fibrillation: A prospective, randomized, open-label, multicenter, exploratory study with blinded, centrally adjudicated endpoint evaluation (RE-CIRCUIT) was conducted in 704 patients who were under stable anticoagulant treatment. The study compared 150 mg twice daily uninterrupted dabigatran etexilate with uninterrupted INR-adjusted warfarin in catheter ablation of paroxysmal or persistent atrial fibrillation. Of the 704 enrolled patients, 317 underwent atrial fibrillation ablation on uninterrupted dabigatran and 318 underwent atrial fibrillation ablation on uninterrupted warfarin. All patients underwent a Trans-oesophageal Echocardiography (TEE) prior to catheter ablation. The primary outcome (adjudicated major bleeding according to ISTH criteria) occurred in 5 (1.6 %) patients in the dabigatran etexilate group and 22 (6.9 %) patients in the warfarin group (risk difference -5.3%; 95% CI -8.4, -2.2; P=0.0009). There was no stroke/systemic embolism/TIA (composite) event in the dabigatran etexilate arm, and one event (TIA) in the warfarin arm from the time of ablation and until 8 weeks post-ablation. The composite incidence of MBEs and thromboembolic events (stroke/systemic embolism/TIA) was lower in the dabigatran etexilate arm (5 [1.6%] vs. 23 [7.2%] patients). This exploratory study demonstrated that dabigatran etexilate was associated with a significant reduction in MBE rate compared with INR-adjusted warfarin in the setting of ablation.
Clinical trials for the prevention of thromboembolism in patients with prosthetic heart valves: A phase II study examined dabigatran etexilate and warfarin in a total of 252 patients with recent mechanical heart valve replacement surgery (i.e. within the current hospital stay) and in patients who received a mechanical heart valve replacement more than three months ago. More thromboembolic events (mainly strokes and asymptomatic prosthetic valve thrombosis) and more bleeding events were observed with dabigatran etexilate than with warfarin. In the early post-operative patients, major bleeding manifested predominantly as haemorrhagic pericardial effusions, specifically in patients who started dabigatran etexilate early (i.e. on Day 3) after heart valve replacement surgery.
Clinical trials in treatment of acute deep vein thrombosis (DVT) and/or pulmonary embolism (PE): Clinical evidence has demonstrated dabigatran etexilate to be an effective and safe treatment for DVT and/or PE in two multi-center, randomised, double blind, parallel-group, replicate studies RE-COVER and RE-COVER II. These studies compared dabigatran etexilate (150 mg bid) with warfarin (target INR 2.0-3.0) in patients with acute DVT and/or PE. The primary objective of these studies was to determine if dabigatran was non-inferior to warfarin in reducing the occurrence of the primary endpoint which was the composite of recurrent symptomatic DVT and/or PE and related deaths within the 6 month acute treatment period.
In the pooled RE-COVER and RE-COVER II studies, a total of 5,153 patients were randomized and 5,107 were treated. The index events at baseline: DVT - 68.5%, PE -22.2%, PE and DVT - 9.1%. The most frequent risk factors were history of DVT and/or PE - 21.5%, surgery/trauma -18.1%, venous insufficiency - 17.6%, and prolonged immobilisation -14.6%. Patients' baseline characteristics: mean age was 54.8 years, males 59.5%, Caucasian 86.1%, Asian 11.8%, blacks 2.1%. The co-morbidities included: hypertension 35.5%, diabetes mellitus 9.0%, CAD 6.8% and gastric or duodenal ulcer 4.1%.
The duration of treatment with fixed dose of dabigatran was 174.0 days without coagulation monitoring. For patients randomized to warfarin, the median time in therapeutic range (INR 2.0 to 3.0) was 60.6%. Concomitant medications included vasodilators 28.5%, agents acting on the renin-angiotensin system 24.7%, lipids lowering agents 19.1%, beta-blockers 14.8%, calcium channel blockers 9.7%, NSAIDs 21.7%, aspirin 9.2%, antiplatelet agents 0.7%, P-gp inhibitors 2.0% (verapamil -1.2% and amiodarone -0.4%).
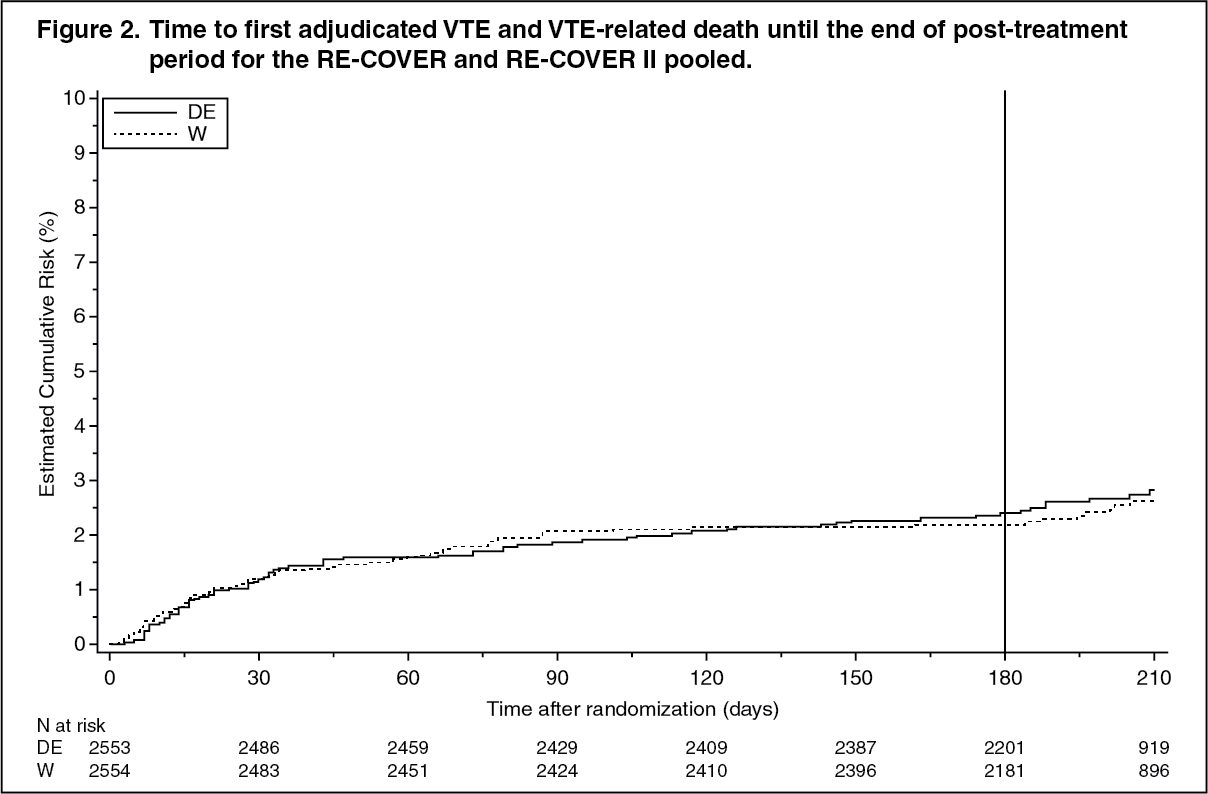
Two trials in patients presenting with acute DVT and/or PE treated initially for at least 5 days of parenteral therapy, RE-COVER and RE-COVER II, demonstrated that treatment with dabigatran etexilate 150 mg twice daily was non-inferior to the treatment with warfarin (p values for non-inferiority: RE-COVER p<0.0001, RECOVER II p=0.0002). Bleeding events (MBEs, MBE/CRBEs and any bleeding) were significantly lower in patients receiving dabigatran etexilate 150 mg twice daily as compared with those receiving warfarin. (See Figure 2 and Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image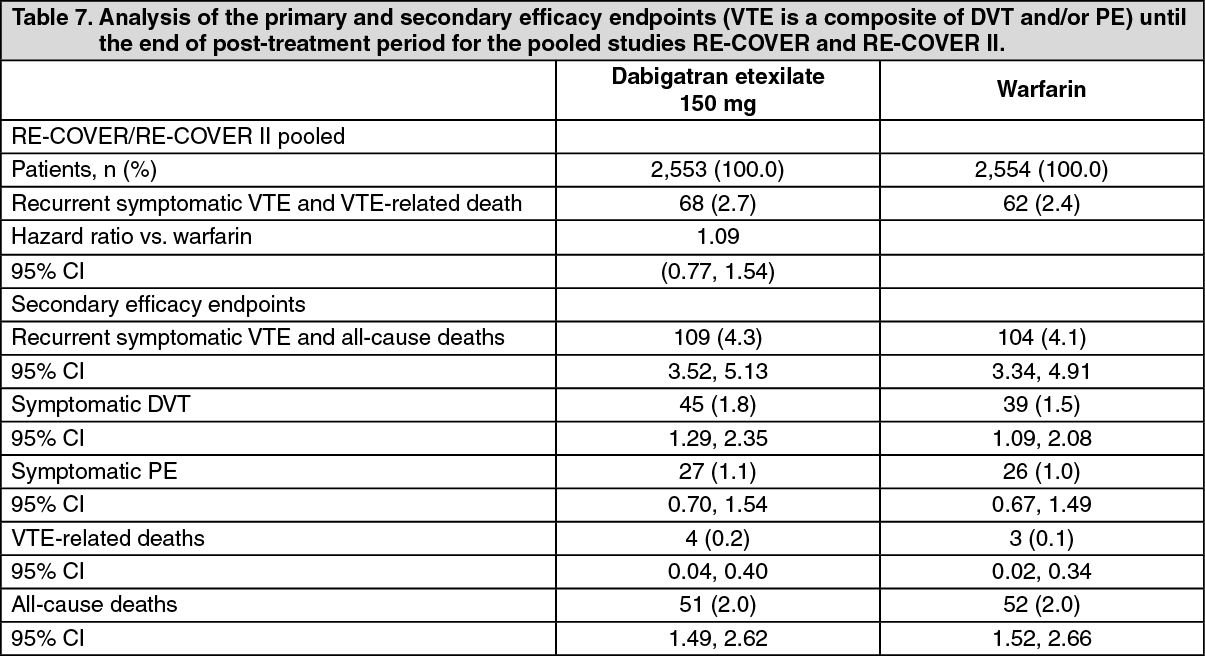 Click on icon to see table/diagram/image
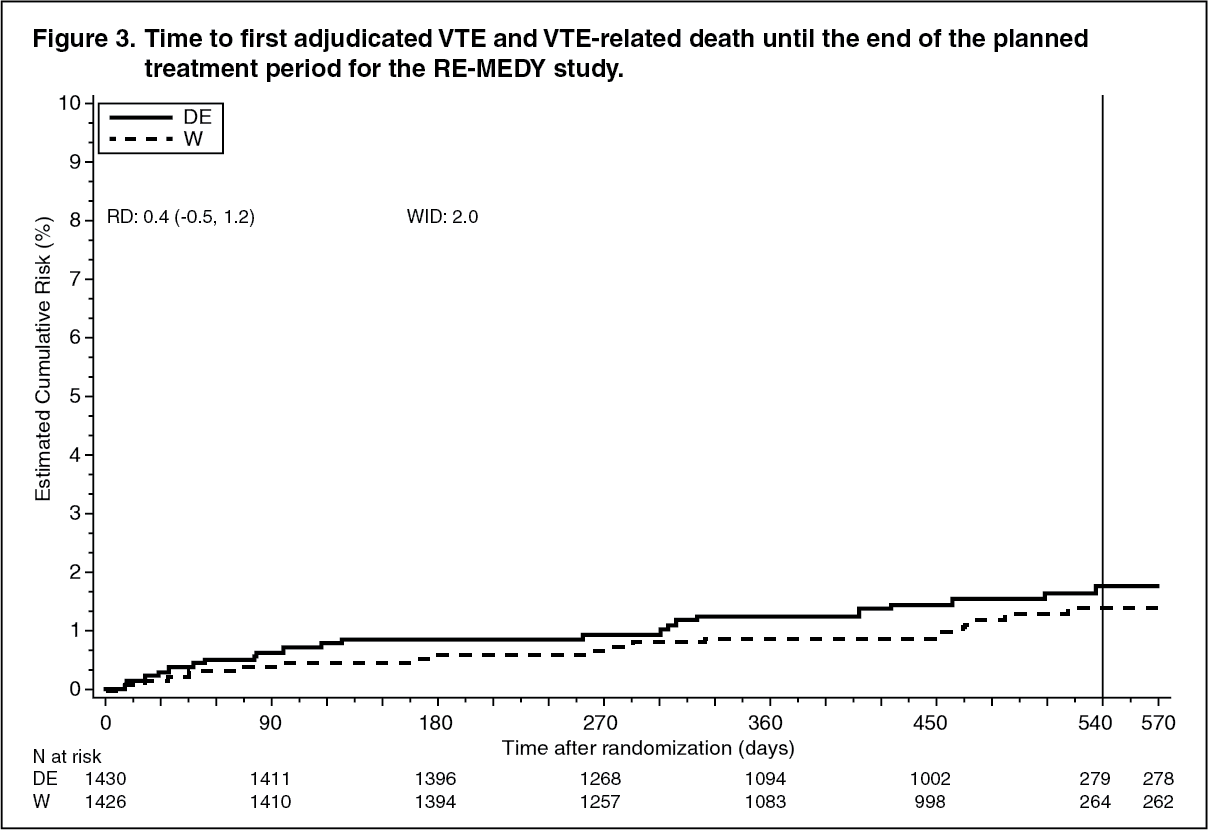
Click on icon to see table/diagram/imageClinical trials in Prevention of recurrent of deep vein thrombosis (DVT) and/or pulmonary embolism (PE): Clinical evidence has demonstrated dabigatran etexilate to be an effective and safe treatment for recurrent DVT and/or PE. Two randomized, parallel group, double-blind studies were performed in patients previously treated with anticoagulation therapy. RE-MEDY, warfarin controlled study, enrolled patients already treated for 3 to 12 months with the need for further anticoagulant treatment and RE-SONATE, the placebo controlled study, enrolled patients already treated for 6 to 18 months with Vitamin K inhibitors.
The objective of the RE-MEDY study was to compare the safety and efficacy of oral dabigatran etexilate (150 mg bid) to warfarin (target INR 2.0-3.0) for the long-term treatment and prevention of recurrent, symptomatic DVT and/or PE. A total of 2,866 patients were randomized and 2,856 patients were treated. The index events at baseline: DVT - 65.1%, PE - 23.1%, PE and DVT -11.7%. Patients' baseline characteristics: mean age 54.6 years, males 61.0%, Caucasian 90.1%, Asian 7.9%, blacks 2.0%. Co-morbidities included hypertension 38.6 %, diabetes mellitus 9.0%, CAD 7.2 % and gastric or duodenal ulcer 3.8 %. Concomitant medications: agents acting on the renin-angiotensin system 27.9 %, vasodilators 26.7%, lipid lowering agents 20.6%, NSAIDs 18.3%, beta-blockers 16.3%, calcium channel blockers 11.1%, aspirin 7.7%, P-gp inhibitors 2.7% (verapamil 1.2% and amiodarone 0.7%), antiplatelets 0.9%. Duration of dabigatran etexilate treatment ranged from 6 to 36 months (median - 534.0 days). For patients randomized to warfarin, the median time in therapeutic range (INR 2.0-3.0) was 64.9%.
RE-MEDY demonstrated that treatment with dabigatran etexilate 150 mg twice daily was non-inferior to warfarin (p=0.0135 for non-inferiority). Bleeding events (MBEs/CRBEs; any bleeding) were significantly lower in patients receiving dabigatran etexilate as compared with those receiving warfarin.
As in the pooled RE-COVER/RE-COVER II studies, in RE-MEDY concomitant use of P-gp inhibitors was reported by few patients (2.7%); verapamil (1.2%) and amiodarone (0.7%) were the most frequent. In the pooled acute VTE treatment studies, concomitant use of P-gp inhibitors was reported by few patients (2.0%); most frequent were verapamil (1.2% overall) and amiodarone (0.4% overall). (See Figure 3.)
 Click on icon to see table/diagram/image
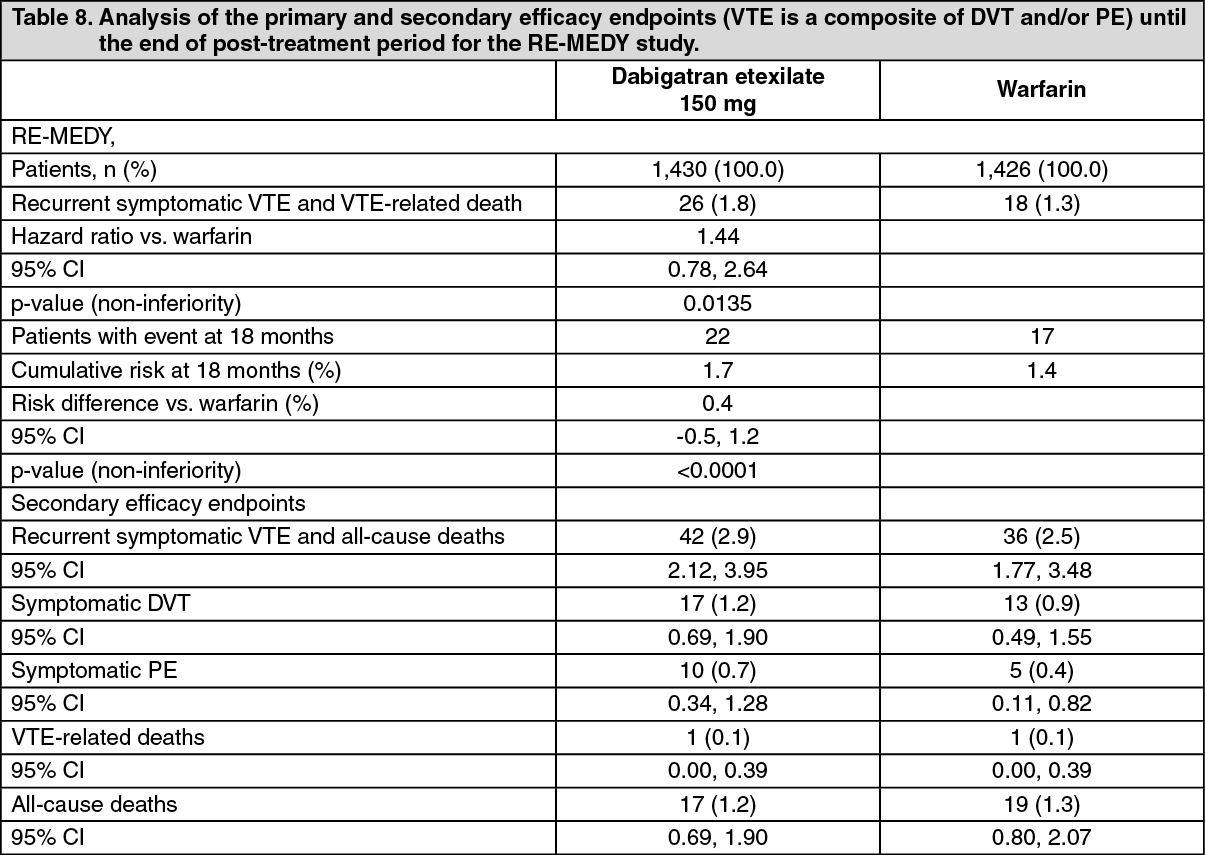
Click on icon to see table/diagram/imageTable 8 displays details of key results of the RE-MEDY study. (See Table 8.)
 Click on icon to see table/diagram/image
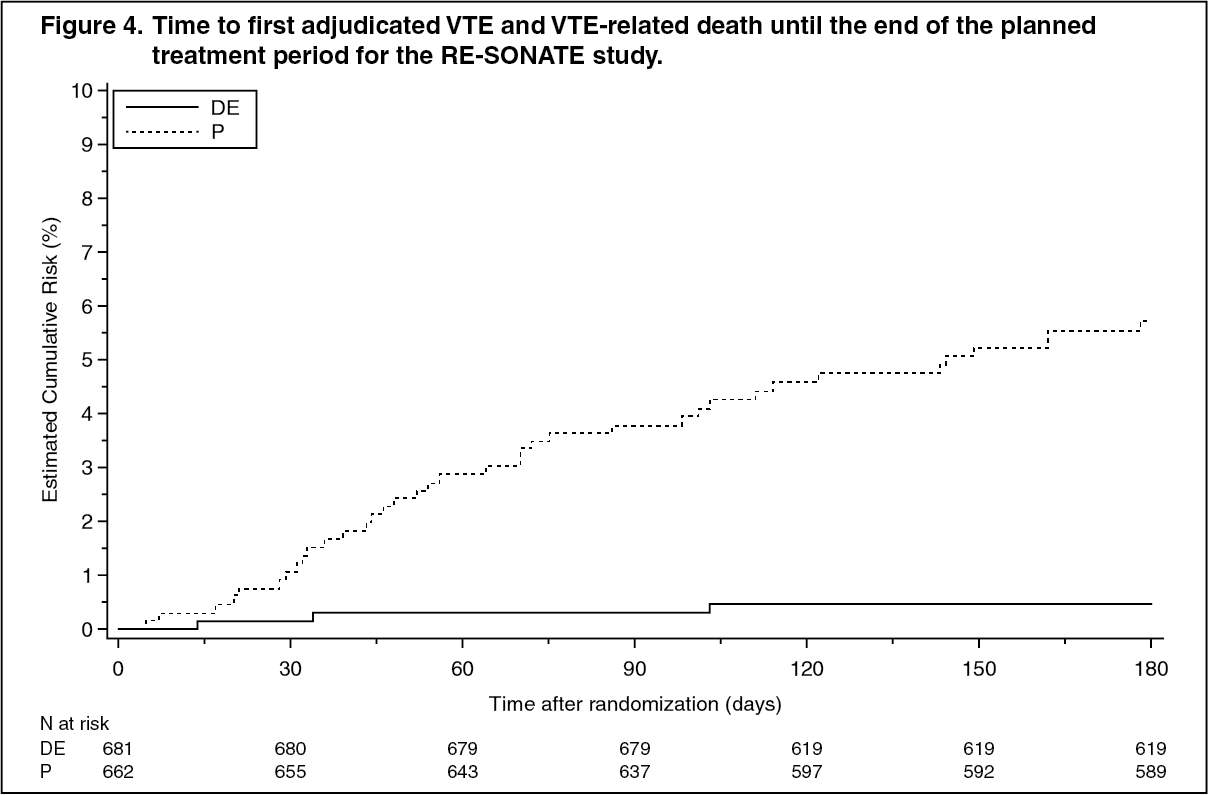
Click on icon to see table/diagram/imageThe objective of the RE-SONATE study was to evaluate superiority of dabigatran etexilate versus placebo for the prevention of recurrent symptomatic DVT and/or PE in patients who had already completed 6 to 18 months of treatment with VKA. The intended therapy was 6 months dabigatran etexilate 150 mg twice daily without need for monitoring.
The index events at baseline: DVT 64.5%, PE 27.8%, PE and DVT 7.7%. A total of 1,353 patients were randomized and 1,343 patients treated. Patients' baseline characteristics: mean age 55.8 years, males 55.5%, Caucasian 89.0%, Asian 9.3%, blacks 1.7%. Co-morbidities included hypertension 38.8%, diabetes mellitus 8.0%, CAD 6.0 % and gastric or duodenal ulcer 4.5%. Concomitant medications: agents acting on the renin-angiotensin system 28.7%, vasodilators 19.4%, lipid lowering agents 17.9%, beta-blockers 18.5%, calcium channel blockers 8.9%, NSAIDs 12.1%, aspirin 8.3%, antiplatelets 0.7% and P-gp inhibitors 1.7% (verapamil 1.0% and amiodarone 0.3%).
RE-SONATE demonstrated dabigatran etexilate was superior to placebo for the prevention of recurrent symptomatic DVT/PE events including unexplained deaths, with a risk reduction of 92% during the treatment period (p<0.0001). All secondary and sensitivity analyses of the primary endpoint and all secondary endpoints showed superiority of dabigatran etexilate over placebo. The rates of MBEs and the combination of MBEs/CRBEs were significantly higher in patients receiving dabigatran etexilate as compared with those receiving placebo.
The study included observational follow-up for 12 months after the conclusion of treatment. After discontinuation of study medication the effect was maintained until the end of the follow-up, indicating that the initial treatment effect of dabigatran etexilate was sustained. No rebound effect was observed. At the end of the follow-up VTE events in patients treated with dabigatran etexilate was 6.9% vs. 10.7% among the placebo group (hazard ratio 0.61 (0.42, 0.88), p=0.0082). (See Figure 4.)
 Click on icon to see table/diagram/image
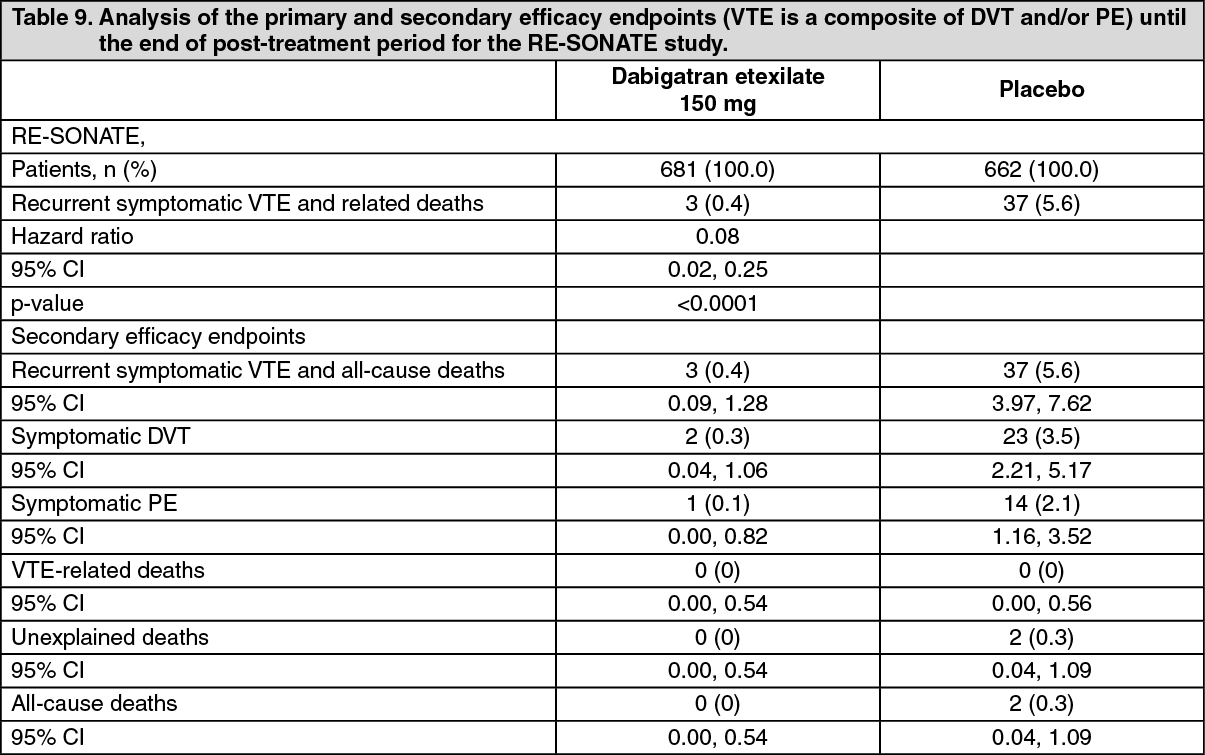
Click on icon to see table/diagram/imageTable 9 displays details of key results of the RE-SONATE study. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOther Measures Evaluated: Treatment of acute deep vein thrombosis (DVT) and/or pulmonary embolism (PE) and prevention of recurrent deep vein thrombosis (DVT) and/or pulmonary embolism (PE): In the three active controlled studies, a higher rate of MI was reported in patients who received dabigatran etexilate than in those who received warfarin: 0.4% vs. 0.2% in the short-term RE-COVER and RE-COVER II studies; and 0.8% vs. 0.1% in the long-term RE-MEDY trial. The increase was statistically significant in this study (p=0.022).
In the RE-SONATE study, which compared dabigatran etexilate to placebo, the rate of MI was 0.1% for patients who received dabigatran etexilate and 0.2% for patients who received placebo.
Liver Function Tests: Treatment of acute deep vein thrombosis (DVT) and/or pulmonary embolism (PE) and prevention of recurrent deep vein thrombosis (DVT) and/or pulmonary embolism (PE): In the active controlled studies RE-COVER, RE-COVER II and RE-MEDY, potential abnormalities of liver function tests (LFT) occurred with a comparable or lower incidence in dabigatran etexilate vs. warfarin treated patients. In RE-SONATE, there was no marked difference between the dabigatran- and placebo groups with regard to possible clinically significant abnormal LFT values.
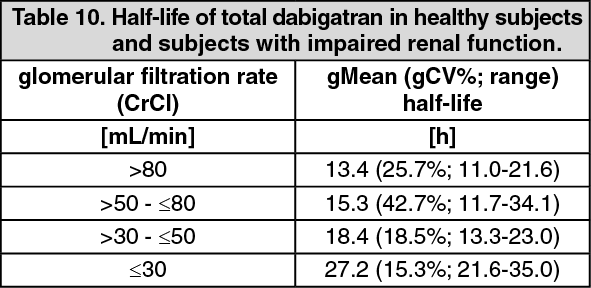
Pharmacokinetics: After oral administration of dabigatran etexilate in healthy volunteers, the pharmacokinetic profile of dabigatran in plasma is characterized by a rapid increase in plasma concentrations with peak concentration (Cmax) attained within 0.5 and 2.0 hours post administration. Cmax and the area under the plasma concentration-time curve (AUC) were dose proportional. After Cmax, plasma concentrations of dabigatran showed a biexponential decline with a mean terminal half-life of approximately 11 hours in healthy elderly subjects. After multiple doses a terminal half-life of about 12-14 hours was observed. The half-life was independent of dose. However, half-life is prolonged if renal function is impaired as shown as follows, in Table 10. (See Table 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe absolute bioavailability of dabigatran following oral administration of dabigatran etexilate as HPMC capsule was approximately 6.5 %.
Food does not affect the bioavailability of dabigatran etexilate but delays the time to peak plasma concentrations by 2 hours.
The oral bioavailability may be increased by about 1.4-fold (+37%) compared to the reference capsule formulation when the pellets are taken without the HPMC capsule shell. Hence, the integrity of the HPMC capsules should always be preserved in clinical use to avoid unintentionally increased bioavailability of dabigatran etexilate. Therefore, patients should be advised not to open the capsules and taking the pellets alone (e.g. sprinkled over food or into beverages) (see "Dosage & Administration").
A study evaluating post-operative absorption of dabigatran etexilate, 1-3 hours following surgery, demonstrated relatively slow absorption compared with that in healthy volunteers, showing a smooth plasma concentration-time profile without high peak plasma concentrations. Peak plasma concentrations are reached at 6 hours following administration, or at 7 to 9 hours following surgery (BISTRO Ib). It is noted however that contributing factors such as anesthesia, gastrointestinal paresis, and surgical effects will mean that a proportion of patients will experience absorption delay independent of the oral drug formulation. Although this study did not predict whether impaired absorption persists with subsequent doses, it was demonstrated in a further study that slow and delayed absorption is usually only present on the day of surgery. On subsequent days absorption of dabigatran is rapid with peak plasma concentrations attained 2 hours after drug administration.
Metabolism and excretion of dabigatran were studied following a single intravenous dose of radiolabeled dabigatran in healthy male subjects. After an intravenous dose, the dabigatran-derived radioactivity was eliminated primarily in the urine (85%). Faecal excretion accounted for 6% of the administered dose. Recovery of the total radioactivity ranged from 88 - 94 % of the administered dose by 168 hours post dose.
After oral administration, dabigatran etexilate is rapidly and completely converted to dabigatran, which is the active form in plasma. The cleavage of the prodrug dabigatran etexilate by esterase-catalysed hydrolysis to the active principle dabigatran is the predominant metabolic reaction. Dabigatran is subject to conjugation forming pharmacologically active acylglucuronides. Four positional isomers, 1-O, 2-O, 3-O, 4-O-acylglucuronide exist, each accounts for less than 10% of total dabigatran in plasma. Traces of other metabolites were only detectable with highly sensitive analytical methods. Dabigatran is eliminated primarily in the unchanged form in the urine, at a rate of approximately 100 ml/min corresponding to the glomerular filtration rate.
Low (34-35%) concentration independent binding of dabigatran to human plasma proteins was observed. The volume of distribution of dabigatran of 60 - 70 L exceeded the volume of total body water indicating moderate tissue distribution of dabigatran.
Special populations: Renal impairment: The exposure (AUC) of dabigatran after the oral administration of dabigatran etexilate in a phase 1 study was approximately 3-fold higher in volunteers with moderate renal insufficiency (CrCL between 30-50ml/min) than in those without renal insufficiency.
In a small number of volunteers with severe renal insufficiency (CrCL 10 - 30 ml/min), the exposure (AUC) to dabigatran was approximately 6 times higher and the half-life approximately 2 times longer than that observed in a population without renal insufficiency (see "Dosage & Administration" and "Contraindications").
Clearance of dabigatran by hemodialysis was investigated in patients with end-stage renal disease (ESRD) without atrial fibrillation. Dialysis was conducted with 700 mL/min dialysate flow rate, four hour duration, a blood flow rate of either 200 mL/min or 350 - 390 mL/min. This resulted in a removal of 50% or 60% of free- or total dabigatran concentrations, respectively. The amount of drug cleared by dialysis is proportional to the blood flow rate up to a blood flow rate of 300ml/min. The anticoagulant activity of dabigatran decreased with decreasing plasma concentrations and the PK/PD relationship was not affected by the procedure.
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: The median CrCL in RE-LY was 68.4 ml/min. Almost half (45.8 %) of the RE-LY patients had a CrCL > 50-<80 ml/min. Patients with moderate renal impairment (CrCL between 30-50 ml/min) had on average 2.29-fold and 1.81-fold higher pre- and post-dose dabigatran plasma concentrations, respectively, when compared with patients without renal impairment (CrCL ≥80 ml/min).
Treatment of acute deep vein thrombosis (DVT) and/or pulmonary embolism (PE): The median CrCl in the RE-COVER study was 100.3 mL/min. 21.7% of patients had mild renal impairment (CrCl > 50-< 80 mL/min) and 4.5% of patients had a moderate renal impairment (CrCl between 30-50mL/min). Patients with mild and moderate renal impairment had on average 1.7-fold and 3.4-fold higher steady state dabigatran trough concentrations compared with patients with CrCl > 80 mL/min. Similar values for CrCl were found in RE-COVER II.
Prevention of recurrent deep vein thrombosis (DVT) and/or pulmonary embolism (PE): The median CrCl in the RE-MEDY and RE-SONATE studies were 99.0 mL/min and 99.7 mL/min respectively. 22.9 % and 22.5% of the patients had a CrCl > 50-< 80 mL/min, and 4.1% and 4.8% had a CrCl between 30-50 mL/min in the RE-MEDY and RE-SONATE studies.
Elderly: Specific pharmacokinetic studies with elderly subjects in phase 1 studies showed an increase of 1.4- to 1.6-fold (+40 to 60%) in the AUC and of more than 1.25-fold (+25 %) in Cmax compared to young subjects.
The AUCτ,ss and Cmax,ss in male and female elderly subjects (> 65 y) were approximately 1.9 fold and 1.6-fold higher for elderly females compared to young females and 2.2 and 2.0 fold higher for elderly males than in male subjects of 18 - 40 years of age.
The observed increase of dabigatran exposure correlated with the age-related reduction in creatinine clearance.
The effect by age on exposure to dabigatran was confirmed in the RE-LY study with an about 1.3-fold (+31%) higher trough concentration for subjects ≥ 75 years and by about 22 % lower trough level for subjects <65 years compared to subjects of age between 65 and 75 years.
Hepatic insufficiency: No change in dabigatran exposure was seen in 12 subjects in a phase 1 study with moderate hepatic insufficiency (Child Pugh B) compared to 12 controls.
Primary prevention of venous thromboembolic events in adult patients who have undergone elective total hip replacement surgery or total knee replacement surgery: Patients with moderate and severe hepatic impairment (Child-Pugh classification B and C) or liver disease expected to have any impact on survival or with elevated liver enzymes ≥ 2 Upper Limit Normal (ULN) were excluded in clinical trials.
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: Patients with active liver disease including but not limited to the persistent elevation of liver enzymes ≥ 2 Upper Limit Normal (ULN), or hepatitis A, B or C were excluded in clinical trials.
Treatment of acute deep vein thrombosis (DVT) and/or pulmonary embolism (PE): Patients with moderate and severe hepatic impairment (Child-Pugh classification B and C) or liver disease expected to have any impact on survival or with elevated liver enzymes ≥ 2 Upper Limit Normal (ULN) were excluded in clinical trials.
Prevention of recurrent deep vein thrombosis (DVT) and/or pulmonary embolism (PE): Patients with moderate and severe hepatic impairment (Child-Pugh classification B and C) or liver disease expected to have any impact on survival or with elevated liver enzymes ≥ 2 Upper Limit Normal (ULN) were excluded in clinical trials.
Body weight: The dabigatran trough concentrations were about 20% lower in patients with a BW > 100 kg compared with 50 - 100 kg. The majority (80.8%) of the subjects were in the ≥ 50 kg and < 100 kg category with no clear difference detected. Limited data in patients ≤ 50 kg are available.
Gender: Primary prevention of venous thromboembolic events in adult patients who have undergone elective total hip replacement surgery or total knee replacement surgery: Drug exposure in the primary VTE prevention studies was about 1.4- to 1.5-fold (+40 % to 50 %) higher in female patients. This finding had no clinical relevance.
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: In atrial fibrillation patients females had on average 1.3-fold (+30 %) higher trough and post-dose concentrations. This finding had no clinical relevance.
Ethnic origin: The pharmacokinetics of dabigatran was investigated in Caucasian and Japanese volunteers after single and multiple doses. Ethnic origin does not affect the pharmacokinetics of dabigatran in a clinically relevant manner.
Limited pharmacokinetic data in black patients are available which suggest no relevant differences.
Pharmacokinetic interactions: In vitro interaction studies did not show any inhibition or induction of cytochrome P450. This has been confirmed by in vivo studies in healthy volunteers, who did not show any interaction between dabigatran etexilate treatment and the following drugs: atorvastatin (CYP3A4) and diclofenac (CYP2C9).
Atorvastatin: When dabigatran etexilate was coadministered with atorvastatin, a CYP3A4 substrate, exposure of atorvastatin, atorvastatin metabolites and of dabigatran were unchanged indicating a lack of interaction.
Diclofenac: When dabigatran etexilate was coadministered with diclofenac, a CYP2C9 substrate, pharmacokinetics of both drugs remained unchanged indicating a lack of interaction between dabigatran etexilate and diclofenac.
P-gp inhibitor / inducer interactions: The pro-drug dabigatran etexilate but not dabigatran is a substrate of the efflux transporter P-glycoprotein (P-gp). Therefore co-medications with P-gp transporter inhibitors and inducers have been investigated.
Co-medication with P-gp inhibitors: Amiodarone: When dabigatran etexilate was coadministered with a single oral dose of 600 mg amiodarone, the extent and rate of absorption of amiodarone and its active metabolite DEA were essentially unchanged. The dabigatran AUC and Cmax were increased by about 1.6-fold and 1.5-fold (+60 % and 50 %), respectively.
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: In the population pharmacokinetics study from RE-LY, no important changes in dabigatran trough levels were observed in patients who received amiodarone (see "Interactions").
Dronedarone: When dabigatran etexilate and dronedarone were given at the same time total dabigatran AUC0-∞ and Cmax values increased by about 2.4-fold and 2.3-fold (+136 % and 125%), respectively, after multiple dosing of 400 mg dronedarone bid, and about 2.1-fold and 1.9-fold (+114% and 87%), respectively, after a single dose of 400 mg. The terminal half-life and renal clearance of dabigatran were not affected by dronedarone. When single and multiple doses of dronedarone were given 2 h after dabigatran etexilate, the increases in dabigatran AUC0-∞ were 1.3-fold and 1.6 fold, respectively.
Verapamil: When dabigatran etexilate was coadministered with oral verapamil, the Cmax and AUC of dabigatran were increased depending on timing of administration and formulation of verapamil.
The greatest elevation of dabigatran exposure was observed with the first dose of an immediate release formulation of verapamil administered one hour prior to dabigatran etexilate intake (increase of Cmax by about 2.8-fold (+180%) and AUC by about 2.5-fold (+150%)). The effect was progressively decreased with administration of an extended release formulation (increase of Cmax by about 1.9-fold (+90%) and AUC by about 1.7-fold (+70%)) or administration of multiple doses of verapamil (increase of Cmax by about 1.6-fold (+60%) and AUC by about 1.5-fold (+50%)). This can be explained by the induction of P-gp in the gut by chronic verapamil treatment.
There was no meaningful interaction observed when verapamil was given 2 hours after dabigatran etexilate (increase of Cmax by about 10% and AUC by about 20%). This is explained by completed dabigatran absorption after 2 hours (see "Dosage & Administration").
No data are available for the parenteral application of verapamil; based on the mechanism of the interaction, no meaningful interaction is expected.
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: In the population pharmacokinetics study from RE-LY, no important changes in dabigatran trough levels were observed in patients who received verapamil (see "Interactions").
Ketoconazole: Systemic ketoconazole increased total dabigatran AUC0-∞ and Cmax values by about 2.4-fold (+138% and 135%), respectively, after a single dose of 400 mg, and about 2.5-fold (+153% and 149%), respectively, after multiple dosing of 400 mg ketoconazole qd. The time to peak, terminal half-life and mean residence time were not affected by ketoconazole.
Clarithromycin: When clarithromycin 500 mg twice daily was administered together with dabigatran etexilate a modest PK-interaction was observed (increased of Cmax by about 15 % and AUC by about 19%).
Quinidine: Quinidine was given as 200 mg dose every 2nd hour up to a total dose of 1000 mg. Dabigatran etexilate was given bid over 3 consecutive days, on the 3rd day either with or without quinidine. Dabigatran AUCτ,ss and Cmax,ss were increased on average by about 1.5-fold (+53 % and 56 %), respectively with concomitant quinidine.
Ticagrelor: When a single dose of 75mg dabigatran etexilate was coadministered simultaneously with a loading dose of 180 mg ticagrelor, the dabigatran AUC and Cmax were increased by 1.73-fold and 1.95-fold (+73% and 95%), respectively. After multiple doses of ticagrelor 90 mg b.i.d. the increase of dabigatran exposure is reduced to 1.56-fold and 1.46-fold (+56% and 46%) for Cmax and AUC, respectively. Concomitant administration of a loading dose of 180 mg ticagrelor and 110 mg dabigatran etexilate (in steady state) increased the dabigatran AUCτ,ss and by Cmax,ss by 1.49-fold and 1.65-fold (+49% and 65%), respectively, compared with dabigatran etexilate given alone. When a loading dose of 180 mg ticagrelor was given 2 hours after 110 mg dabigatran etexilate (in steady state), the increase of dabigatran AUCτ,ss and Cmax,ss was reduced to 1.27-fold and 1.23-fold (+27% and 23%), respectively, compared with dabigatran etexilate given alone. Concomitant administration of 90 mg ticagrelor BID (maintenance dose) with 110 mg dabigatran etexilate increased the adjusted dabigatran AUCτ,ss and Cmax,ss 1.26-fold 1.29-fold, respectively, compared with dabigatran etexilate given alone.
Co-medication with P-gp substrates: Digoxin: When dabigatran etexilate was coadministered with digoxin, a P-gp substrate, no PK-interaction was observed. Neither dabigatran nor the pro-drug dabigatran etexilate is a clinically relevant P-gp inhibitor.
Co-medication with P-gp inducers: Rifampicin: Pre-dosing of the probe inducer rifampicin at a dose of 600 mg qd for 7 days decreased total dabigatran peak and total exposure by 65.5 and 67 %, respectively. The inducing effect was diminished resulting in dabigatran exposure close to the reference by day 7 after cessation of rifampicin treatment. No further increase in bioavailability was observed after another 7 days.
Co-medications with platelet-inhibitors: Acetylsalicylic acid (ASA): The effect of concomitant administration of dabigatran etexilate and acetylsalicylic acid (ASA) on the risk of bleeds was studied in patients with atrial fibrillation in a phase II study in which a randomized ASA coadministration was applied. Based on logistic regression analysis, co-administration of ASA and 150 mg dabigatran etexilate twice daily may increase the risk for any bleeding from 12 % to 18 % and 24% with 81 mg and 325 mg ASA, respectively.
From the data gathered in the phase III study RE-LY it was observed that ASA or clopidogrel co-medication with dabigatran etexilate at dosages of 110 or 150 mg bid may increase the risk of major bleeding. The higher rate of bleeding events by ASA or clopidogrel co-medication was, however, also observed for warfarin.
NSAIDs: NSAIDs given for short-term perioperative analgesia have been shown not to be associated with increased bleeding risk when given in conjunction with dabigatran etexilate. There is limited evidence regarding the use of regular NSAID medication with half-lives of less than 12 hours during treatment with dabigatran etexilate and this has not suggested additional bleeding risk.
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: NSAIDs increased the risk of bleeding in RE-LY in all treatment groups.
Clopidogrel: In a phase I study in young healthy male volunteers, the concomitant administration of dabigatran etexilate and clopidogrel resulted in no further prolongation of capillary bleeding times (CBT) compared to clopidogrel monotherapy. In addition, dabigatran AUCτ,ss and Cmax,ss and the coagulation measures for dabigatran effect, aPTT, ECT or TT (anti FIIa), or the inhibition of platelet aggregation (IPA) as measure of clopidogrel effect remained essentially unchanged comparing combined treatment and the respective mono-treatments. With a loading dose of 300 or 600 mg clopidogrel, dabigatran AUCτ,ss and Cmax,ss were increased by about 1.3- to 1.4-fold (+30 to 40%) (see previously mentioned subsection on ASA).
Antiplatelets or other anticoagulants: The concomitant use of dabigatran etexilate and antiplatelets or other anticoagulants may increase the risk of bleeding (see "Precautions").
Co-medication with selective serotonin re-uptake inhibitors: SSRIs increased the risk of bleeding in RE-LY in all treatment groups.
Co-medication with gastric pH-elevating agents: The changes in dabigatran exposure determined by population pharmacokinetic analysis caused by PPIs and antacids were not considered clinically relevant because the magnitude of the effect were minor (fractional decrease in bioavailability not significant for antacids and 14.6% for PPIs).
Pantoprazole: When dabigatran etexilate was coadministered with pantoprazole, a decrease in dabigatran area under the plasma concentration - time curve of approximately 30 % was observed. Pantoprazole and other proton-pump inhibitors were co-administered with dabigatran etexilate in clinical trials and no effects on bleeding or efficacy were observed.
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation: In the phase III study, RE-LY, PPI co-medication did not result in lower trough levels and on average only slightly reduced post-dose concentrations (- 11%). Accordingly, PPI co-medication seemed to be not associated with a higher incidence of stroke or SEE, especially in comparison with warfarin, and hence, the reduced bioavailability by pantoprazole co-administration seemed to be of no clinical relevance.
Ranitidine: Ranitidine administration together with dabigatran etexilate had no meaningful effect on the extent of absorption of dabigatran.