Clinically significant adverse reactions: Congestive heart failure, myocardial infarction, angina pectoris (0.1% to less than 5% for each), and ventricular tachycardia (incidence unknown): Congestive heart failure, myocardial infarction, angina pectoris, and ventricular tachycardia may occur. If any signs of these adverse reactions are observed, the drug should be discontinued, and appropriate measures should be taken.
Hemorrhage: Intracranial hemorrhage, such as cerebral hemorrhage (0.1% to less than 5%): Intracranial hemorrhage, such as cerebral hemorrhage (early symptoms of intracranial hemorrhage include headache, nausea, vomiting, consciousness disturbance, and hemiplegia), may occur. If any such symptoms occur, the drug should be discontinued and appropriate measures should be taken.
Pulmonary hemorrhage (less than 0.1%), hemorrhage in the digestive tract, epistaxis, and bleeding in the ocular fundus (0.1% to less than 5% for each): Pulmonary hemorrhage, hemorrhage in the digestive tract, epistaxis, and bleeding in the ocular fundus may occur. If any such symptoms occur, the drug should be discontinued and appropriate measures should be taken.
Gastric or duodenal ulcers (0.1% to less than 5%): Gastric or duodenal ulcers with hemorrhage may occur. Patients should be closely monitored. If any signs of these adverse reactions are observed, the drug should be discontinued and appropriate measures should be taken.
Pancytopenia, agranulocytosis (both incidence unknown), and thrombocytopenia (0.1% to less than 5%): Pancytopenia, agranulocytosis, and thrombocytopenia may occur. Patients should be closely monitored. If any signs of these adverse reactions are observed, the drug should be discontinued and appropriate measures should be taken.
Interstitial pneumonia (less than 0.1%): Interstitial pneumonia accompanied by fever, cough, dyspnoea, abnormal chest X-rays, and eosinophilia may occur. If any signs of interstitial pneumonia are noted, the drug should be discontinued and appropriate measures should be taken.
Hepatic dysfunction (0.1% to less than 5%) and jaundice (incidence unknown): Hepatic dysfunction, as indicated by elevated AST (GOT), ALT (GPT), ALP, or LDH, and jaundice may occur. Patients should be closely monitored. If signs of hepatic dysfunction are observed, the drug should be discontinued and appropriate measures should be taken.
Acute renal failure (less than 0.1%): Acute renal failure may occur. Patients should be closely monitored, such as by renal function testing. If signs of renal failure are observed, the drug should be discontinued and appropriate measures should be taken.
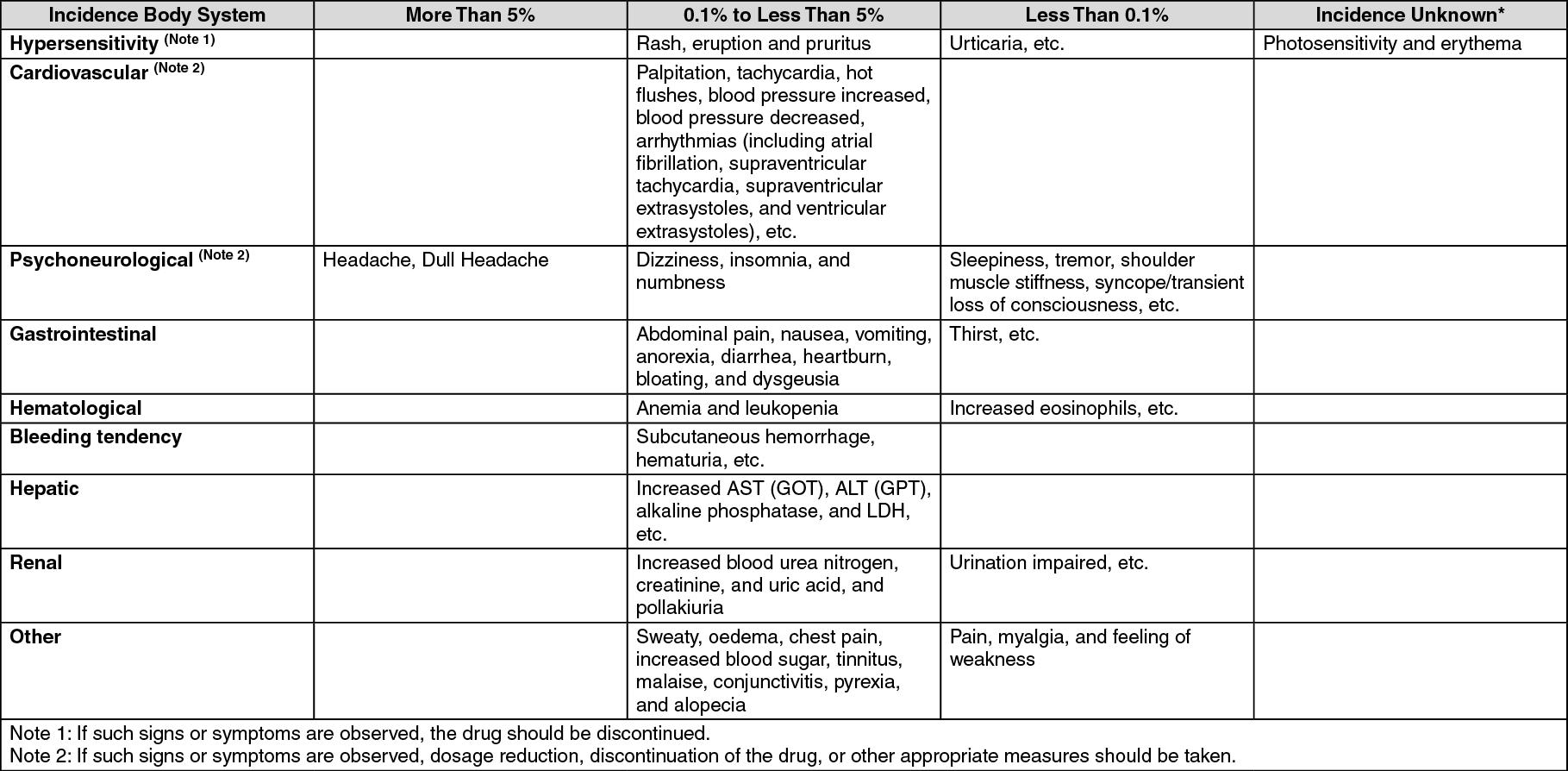
Other adverse reactions: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out