Adult: 15-25 mg given 1 hr before bedtime. Up to 50 mg may be occasionally required.
Oral Alcohol withdrawal syndrome, Anxiety
Adult: 15-30 mg 3 or 4 times daily. Elderly: Initially, 10 mg tid, increase up to 10-20 mg 3 or 4 times daily as necessary.
Special Patient Group
Debilitated patient: Initially, 10 mg tid, increase up to 10-20 mg 3 or 4 times daily as necessary.
Renal Impairment
No dosage adjustment needed.
Administration
May be taken with or without food.
Special Precautions
Patient w/ CV or cerebrovascular disease, acute narrow-angle glaucoma, suicidal tendencies, history of drug abuse or acute alcoholism, myasthenia gravis, chronic pulmonary insufficiency or sleep apnoea. Not intended for treatment of psychoses. Avoid abrupt withdrawal. Hepatic and renal impairment. Elderly or debilitated patient. Pregnancy and lactation.
Adverse Reactions
Sleep and visual disturbances, drowsiness, dizziness, vertigo, lethargy, headache, tremor, ataxia, mild paradoxical reactions (e.g. excitement, stimulation of affect), minor diffuse skin rashes (e.g. morbilliform, maculopapular and urticarial), nausea, oedema, slurred speech, altered libido, GI symptoms. Rarely, transient anterograde amnesia or memory impairment, syncope, leucopenia and hepatic dysfunction including jaundice.
May impair ability to perform hazardous activities requiring mental alertness or physical coordination (e.g. operating machinery, driving).
Monitoring Parameters
Monitor resp and CV status. Periodic monitoring of CBC and LFTs.
Overdosage
Symptoms: Drowsiness, mental confusion, lethargy, ataxia, hypotension, hypotonia, resp depression, coma and very rarely, death. Management: Symptomatic and supportive treatment. If ingestion is recent, induce vomiting and/or gastric lavage. Admin of activated charcoal may reduce absorption. Hypotension may be controlled w/ norepinephrine. Flumazenil may be used as an adjunct for proper management but there is a risk of seizure particularly in long-term benzodiazepine users and in TCA overdose.
Description: Oxazepam is a short-acting benzodiazepine. It increases neuronal membrane permeability to Cl ions by binding to stereospecific benzodiazepine receptors on the postsynaptic GABA neuron w/in the CNS (including the limbic system, reticular formation) and enhancing the GABA inhibitory effects resulting in hyperpolarisation and stabilisation. Pharmacokinetics: Absorption: Well absorbed from the GI tract. Time to peak plasma concentration: Approx 2-3 hr. Distribution: It crosses the placenta and detected in breast milk. Plasma protein binding: Approx 97%. Metabolism: Undergoes hepatic conjugation to produce the major inactive glucuronide metabolite. Excretion: Via urine as inactive glucuronide conjugate. Elimination half-life: Approx 4-15 hr.
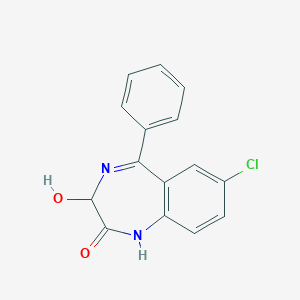
Chemical Structure
Oxazepam Source: National Center for Biotechnology Information. PubChem Database. Oxazepam, CID=4616, https://pubchem.ncbi.nlm.nih.gov/compound/Oxazepam (accessed on Jan. 22, 2020)
Anon. Oxazepam. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 23/04/2014.Buckingham R (ed). Oxazepam. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 23/04/2014.McEvoy GK, Snow EK, Miller J et al (eds). Benzodiazepine General Statement. AHFS Drug Information (AHFS DI) [online]. American Society of Health-System Pharmacists (ASHP). https://www.medicinescomplete.com. Accessed 23/04/2014.McEvoy GK, Snow EK, Miller J et al (eds). Oxazepam. AHFS Drug Information (AHFS DI) [online]. American Society of Health-System Pharmacists (ASHP). https://www.medicinescomplete.com. Accessed 23/04/2014.Oxazepam Capsule (Sandoz Inc.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 23/04/2014.



 Sign Out
Sign Out