In controlled US and international clinical studies, a total of 3210 adult and adolescent patients 12 years and older with allergic rhinitis received treatment with Mometasone Furoate at doses of 50 to 800μg/day. The majority of patients (n = 2103) were treated with 200 μg/day. In controlled US and international clinical studies, a total of 990 pediatric patients (3 to 11 years) with allergic rhinitis received treatment with Mometasone Furoate at doses of 25 to 200μg/day. The majority of patients (n = 720) were treated with 100μg/day. A total of 513 adult and pediatric patients have been treated for one year or longer. Adverse events did not differ significantly based on age, sex, or race. Four percent or less of patients in clinical trials discontinued treatment because of adverse events and the discontinuation rate was similar for the vehicle and active comparators.
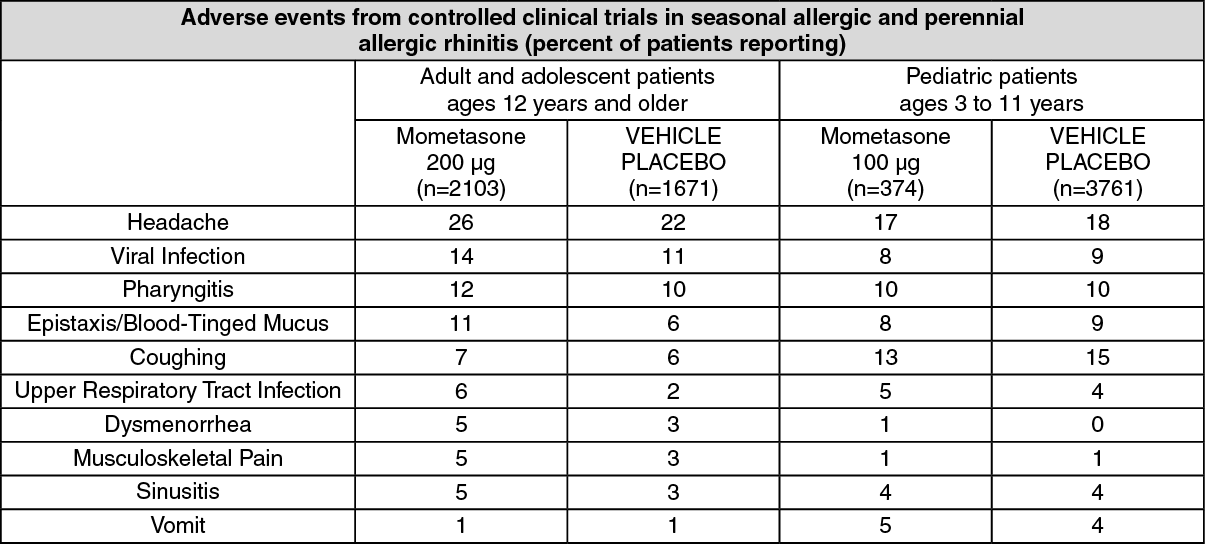
All adverse events (regardless of relationship to treatment) reported by 5% or more of adult and adolescent patients ages 12 years and older who received Mometasone Furoate, 200μg/day and pediatric patients ages 3 to 11 years who received Mometasone Furoate, 100μg/day vs. placebo and that were more common with Mometasone Furoate than placebo, are displayed in table as follows. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Other adverse events which occurred in less than 5% but greater than or equal to 2% of adult and adolescent patients (ages 12 years and older) treated with Mometasone Furoate, 200μg/day (regardless of relationship to treatment), and more frequently than in the placebo group included: arthralgia, asthma, bronchitis, chest pain, conjunctivitis, diarrhea, dyspepsia, earache, flu-like symptoms, myalgia, nausea, and rhinitis.
Other adverse events which occurred in less than 5% but greater than or equal to 2% of adult and adolescent patients (ages 3 to 11 years) treated with Mometasone Furoate, 100μg/day (regardless of relationship to treatment), and more frequently than in the placebo group included: diarrhea, nasal irritation, otitis media, wheezing.
The adverse event (regardless of relationship to treatment) reported by 5% of pediatric patients ages 2 to 5 years who received Mometasone Furoate 100μg/day in a clinical trial vs. placebo including 56 subjects (28 each Mometasone Furoate and placebo) and that was more common with Mometasone Furoate than placebo, included: upper respiratory tract infection (7% vs. 0%, respectively). The other adverse event which occurred in less than 5% but greater than or equal to 2% of mometasone furoate pediatric patients ages 2 to 5 years treated with 100μg doses vs. placebo (regardless of relationship to treatment) and more frequently than in the placebo group included: skin trauma.
Nasal ulcers and nasal and oral candidiasis were also reported in patients treated with Mometasone Furoate primarily in patients treated for longer than 4 weeks.
The following adverse reactions have been identified during the post-marketing period for Mometasone Furoate: nasal burning and irritation, anaphylaxis and angioedema, disturbances in taste and smell and nasal septal perforation. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
In controlled clinical studies, the types of adverse events observed in patients with nasal polyps were similar to those observed for patients with allergic rhinitis.



 Sign Out
Sign Out