Adult: Treatment-experienced patients w/ CCR5-tropic infection: In combination w/ other antiretrovirals that are not potent CYP3A inhibitors or inducers (e.g. ritonavir-boosted tipranavir, nevirapine, enfuvirtide, raltegravir, NRTIs): 300 mg bid.
Hypersensitivity. Lactation. Concomitant use w/ potent CYP3A enzyme inhibitors and inducers in patients w/ severe (CrCl <30 mL/min) renal impairment or ESRD.
Special Precautions
Patient w/ severe CV disease, history of postural hypotension. Hepatic (e.g. chronic active hepatitis B or C) and renal impairment. Pregnancy. Patients taking potent CYP3A enzyme inhibitors (w/ or w/o potent inducers) or potent CYP3A enzyme inducers (w/o potent inhibitors). Not indicated for use in patients w/ CXCR4- or dual/mixed tropic HIV-1 infection.
This drug may cause dizziness, if affected, do not drive or operate machinery.
Monitoring Parameters
Perform coreceptor tropism testing prior to initiation. Monitor transaminases and bilirubin prior to initiation and periodically during treatment; viral load, CD4 count. Monitor for signs and symptoms of infection, rash, severe skin reactions, hepatitis, and postural hypotension.
Overdosage
Symptoms: Postural hypotension. Management: Supportive treatment including keeping the patient in supine position. Assess vital signs, BP, and ECG. Employ gastric lavage/activated charcoal, or induce emesis to remove unabsorbed drug.
Drug Interactions
Increased plasma concentration w/ CYP3A enzyme inhibitors (e.g. protease inhibitors except ritonavir-boosted tipranavir, delavirdine, ketoconazole, itraconazole, voriconazole, clarithromycin, telithromycin, nefazodone, boceprevir). Decreased plasma concentration w/ CYP3A enzyme inducers (e.g. efavirenz, etravirine, rifampicin, carbamazepine, phenobarbital, phenytoin). Increased risk of CV events w/ medications that lower BP. Potentially Fatal: Increased risk of postural hypotension which may trigger CV events in patients w/ severe renal impairment or ESRD who are taking CYP3A inhibitors and inducers.
Food Interaction
Development of resistance and decreased plasma concentration w/ St. John’s wort.
Action
Description: Maraviroc, a synthetic HIV-1 entry inhibitor, selectively and reversibly antagonises CC chemokine receptor-5 (CCR5) coreceptors found on human CD4+ cells. This prevents interaction of HIV-1 glycoprotein 120 (gp120) and CCR5 necessary for CCR5-tropic HIV-1 to enter cells. Pharmacokinetics: Absorption: Absorbed after oral doses. Bioavailability: 23-33%. Time to peak plasma concentration: 0.5-4 hr. Distribution: Crosses the placenta. Volume of distribution: Approx 194 L. Plasma protein binding: Approx 76%, w/ moderate affinity for albumin and α1-acid glycoprotein. Metabolism: Metabolised in the liver by CYP3A4/5 enzymes to inactive metabolites. Excretion: Via urine (approx 20%, 8% as unchanged drug) and faeces (76%, 25 % as unchanged drug). Terminal elimination half-life: 14-18 hr.
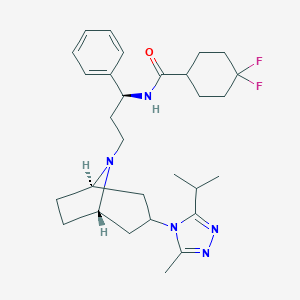
Chemical Structure
Maraviroc Source: National Center for Biotechnology Information. PubChem Database. Maraviroc, CID=3002977, https://pubchem.ncbi.nlm.nih.gov/compound/Maraviroc (accessed on Jan. 21, 2020)
J05AX09 - maraviroc ; Belongs to the class of other antivirals. Used as a direct acting antiviral in the systemic treatment of viral infections.
References
Anon. Maraviroc. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 05/06/2017.Buckingham R (ed). Maraviroc. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 05/06/2017.Joint Formulary Committee. Maraviroc. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 05/06/2017.McEvoy GK, Snow EK, Miller J et al (eds). Maraviroc. AHFS Drug Information (AHFS DI) [online]. American Society of Health-System Pharmacists (ASHP). https://www.medicinescomplete.com. Accessed 05/06/2017.Selzentry Tablet, Film Coated; Solution (ViiV Healthcare Company). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 05/06/2017.



 Sign Out
Sign Out