Levofloxacin hemihydrate.
Tablet: Levocil Tablet 250 mg: Each film coated tablet contains: Levofloxacin hemihydrate USP equivalent to Levofloxacin 250 mg.
Levocil Tablet 500 mg: Each film coated tablet contains: Levofloxacin hemihydrate USP equivalent to Levofloxacin 500 mg.
Infusion: Levocil Infusion 500mg: Each 100ml contains: Levofloxacin hemihydrate U.S.P equivalent to Levofloxacin 500 mg.
Pharmacology: Antibacterial Activity: Levocil is a wide-spectrum antibacterial agent against gram-positive and gram-negative bacteria, including anaerobes. Levocil has shown strong antibacterial activities against
Staphylococcus spp.,
Streptococcus pneumoniae,
Streptococcus pyogenes,
Streptococcus haemolyticus,
Enterobacter spp.,
Escherichia coli,
Klebsiella spp.,
Serratia spp.,
Enterococcus spp.,
Proteus spp., and other glucose non-fermentative gram-negative rods,
Pseudomonas aeruginosa,
Haemophilus influenzae, and
Neisseria gonorrhoeae. Moreover, Levocil has shown antibacterial activity against
Chlamydia trachomatis. Levocil has excellent protective and treatment effects in mice.
Mechanism of Action: The main mechanism of action of Levocil is the inhibition of DNA gyrase. It is two fold stronger than that of ofloxacin. There is not much difference between the MIC and MBC. The activity of Levocil is bactericidal. In the observation of bacterial morphology, bacteriolysis can be seen in the concentration around MIC.
Pharmacokinetics: Distribution in Plasma: Approximately 30-40% of Levofloxacin is bound to serum protein. 500mg once daily multiple dosing with Levofloxacin showed negligible accumulation. There is modest but predictable accumulation of Levofloxacin after doses of 500mg twice daily. Steady-state is achieved within 3 days.
Penetration into tissues and body fluids: Penetration into Bronchial mucosa, Epithelial Lining Fluid (ELF). Maximum Levofloxacin concentrations in bronchial mucosa and epithelial lining fluid were 8.3 ug/ml and 10.8 ug/ml respectively. These were reached approximately one hour after administration.
Penetration into lung tissue: Maximum Levofloxacin concentrations in lung tissue were approximately 11.3 ug/ml and were reached between 4 and 6 hours after administration. The concentration in the lungs consistently exceeded those in plasma.
Metabolism: Levofloxacin is metabolised to a very small extent, the metabolites being desmethyl-levofloxacin and levofloxacin N-oxide. These metabolites account for < 5% of the dose excreted in urine. Levofloxacin is stereochemically stable and does not undergo chiral inversion.
Elimination: Following oral and intravenous administration, Levofloxacin is eliminated relatively slowly from the plasma (t
½ : 6-8 h). Excretion is primarily by the renal route (> 85% of the administered dose). There are no major differences in the pharmacokinetics of Levofloxacin following intravenous and oral administration, suggesting that the oral and intravenous routes are interchangeable.
Tablet: Absorption: Orally administered Levofloxacin is rapidly and almost completely absorbed with peak plasma concentrations being obtained within 1 hr. The absolute bioavailability is approximately 100%. Food has little effect on the absorption of Levofloxacin.
Subjects with renal insufficiency: The pharmacokinetics of Levofloxacin are affected by renal impairment. With decreasing renal function, renal elimination and clearance are decreased, and elimination half-lives increased as shown in the table as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Elderly subjects:
Click on icon to see table/diagram/image
Elderly subjects: There are no significant differences in Levofloxacin kinetics between young and elderly subjects, except those associated with differences in clearance.
Gender differences: Separate analysis for male and female subjects did not show clinical relevant gender differences in Levofloxacin pharmacokinetics.
Tablet: The following infections caused by Staphylococcus spp., Streptococcus pneumoniae, Streptococcus pyogenes, Streptococcus haemolyticus, Enterococcus spp., Peptostreptococcus spp., Neisseria gonorrhoeae, Branhamella catarrhalis, Propionibacterium acnes, Escherichia coli, Citrobacter spp., Salmonella spp., Shigella spp., Klebsiella spp., Enterobacter spp., Serratia spp., Proteus spp., Vibrio cholerae, Pseudomonas aeruginosa, Haemophilus influenzae, Acinetobacter spp., Campylobacter spp., Chlamydia spp., Mycoplasma spp., Legionella spp., are susceptible to levofloxacin.
Pneumonia, chronic bronchitis, diffuse panbronchiolitis, bronchiectasis with infection, secondary infections in chronic respiratory disease.
Laryngopharyngitis, tonsillitis (peritonsillitis, peritonsillar abscess), acute bronchitis.
Pyelonephritis, cystitis, prostatitis, epididymitis, gonococcal urethritis, non-gonococcal urethritis.
Intrauterine infections, cervicitis, uterine adnexitis, bartholinitis.
Folliculitis (including acne pustulosa), furuncle, furunculosis, carbuncle, impetigo contagiosa, hydradenitis, acne conglabata, infectious atheroma, periproctic abscess.
Mastitis, (superficial) secondary infections in traumatic wounds, burns, operative wounds, etc.
Cholecystitis, cholangitis.
Otitis externa, otitis media, sinusitis, suppurative sialadenitis.
Blepharitis, hordeolum, dacryocystitis, conjunctivitis, tarsadenitis.
Bacterial dysentery, infectious enteritis, Salmonella enteritis, cholera.
Periodontitis, pericoronitis, gnathitis.
Infusion: Levocil I.V is used for the treatment of the following bacterial infections in adults when caused by Levofloxacin sensitive bacteria: Community acquired pneumonia.
Complicated urinary tract infections.
Skin and soft tissue infections.
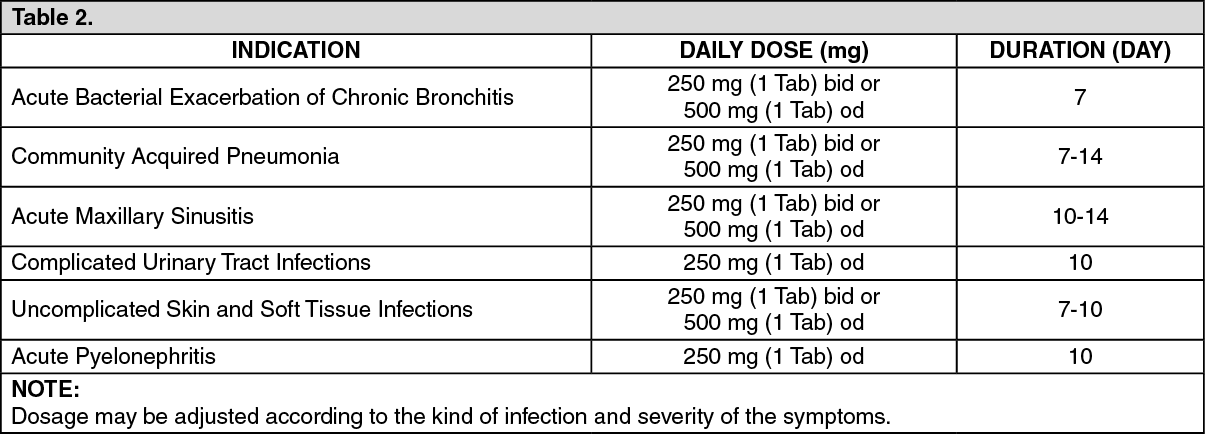
Tablet: The following dose recommendations can be given for Levocil.
Dosage in patients with normal renal functions (Creatinine clearance > 50 ml/min): See Table 2.
Click on icon to see table/diagram/image
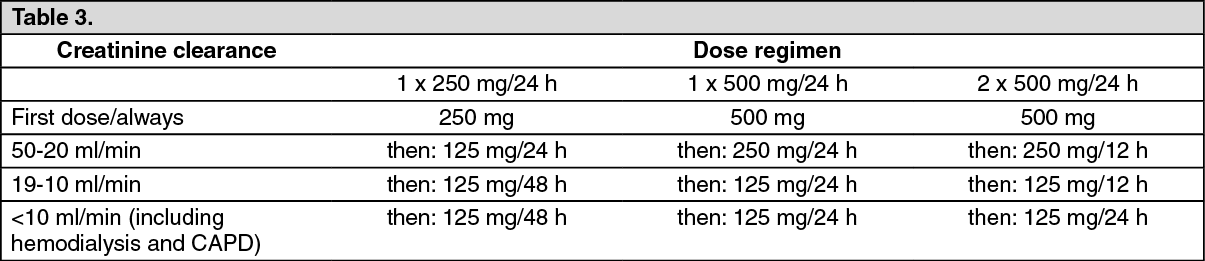
Dosage in patients with impaired renal function (Creatinine clearance ≤ 50 ml/min): See Table 3.
Click on icon to see table/diagram/image
No additional doses are required after hemodialysis or continuous ambulatory peritoneal dialysis (CAPD).
Dosage in elderly: No adjustment of dosage is required in the elderly, other than imposed by consideration of renal function.
Infusion: Levocil I.V 500 mg solution for infusion is administered once or twice daily. The dose is determined by the type and severity of the infection and the sensitivity of the suspected causative pathogen. The following dosage recommendations can be given for patients with normal renal function (creatinine clearance - 50 ml/min):
Pneumonia: 500mg Levofloxacin 1 to 2 times daily.
Urinary Tract Infections: 250 mg Levofloxacin once daily (consideration should be given to increasing the dose in case of severe infection).
Skin and soft tissue infections: 500 mg twice daily.
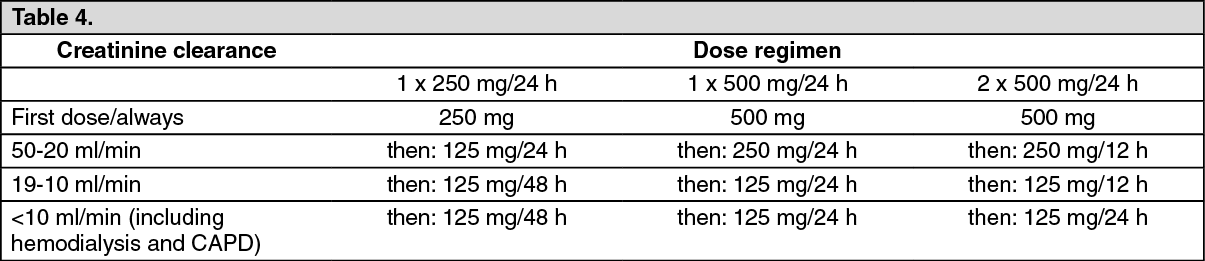
Dosage in patients with impaired renal function (Creatinine clearance ≤ 50 ml/min): As Levofloxacin is eliminated predominantly by the kidneys the dosage should be reduced in patients with renal insufficiency. Further information is given in the following table. (See Table 4.)
Click on icon to see table/diagram/image
Dosage in patients with impaired hepatic function: No dose-reduction is required, because Levofloxacin is not significantly metabolised by the liver.
Method of administration: Tablet:
Levocil tablets should be swallowed without crushing and with
sufficient amount of liquid. They may be divided at the score line to
adapt the dosage. The tablets may be taken during meals or between
meals. Levocil tablets should be taken two hours before iron salts,
antacids and sucralfate administration since reduction of absorption can
occur.
Infusion: Levocil I.V solution for infusion is administered by slow intravenous infusion. The infusion time for 1 bottle Levocil I.V (100 ml solution for infusion with 250mg Levofloxacin) should not be less than 60 minutes. (See also Precautions). According to the patient's condition after some days the treatment may be changed from an initially intravenous infusion into an oral treatment at the same dose.
Levocil I.V solution for infusion is compatible with the following solutions for infusion: 0.9% NaCl solution, 5% dextrose solution, 2.5% dextrose in Ringer solution, combination solutions for parenteral nutrition (amino acids, carbohydrates, electrolytes). Levocil I.V 250mg must not be mixed with heparin or alkaline solutions (e.g. Sodium hydrogen carbonate).
Duration of treatment: The duration of treatment is determined according to the disease process and is not longer than 14 days. As with other anti bacterial agents, treatment with Levocil I.V (infusion, solution or tablets) should be continued for at least 48-72 hours after body temperature has returned to normal or the pathogens have been demonstrably eradicated.
Tablet: Patients with a history of hypersensitivity to any ingredient in this product or to ofloxacin.
Pregnant women or women suspected of being pregnant. (See "Use in Pregnancy & Lactation.")
Children. (See "Use in Children" as follows.)
Infusion: Levocil I.V must not be administered if any of the following conditions applies to the patient or if they belong to any of the following patients groups, because the drug will possibly more harm than help: Hypersensitivity to Levofloxacin or any other quinolone antibiotic.
Patients who suffer from epilepsy.
Patients with a history of tendon disorders related to treatment with an antibiotic of the fluoroquinolone class.
Use in Children: Tablet: Since the product's safety for use by children has not been established, this product should not be administered to children.
Infusion: Levocil must not be administered to children and adolescents as cartilage damage can not be excluded.
Tablet: To prevent the development of resistance, susceptibility to the drug should be determined before use. The duration of use should be limited to the minimum time required for treatment.
Careful Administration: Patients with severe renal disorders.
Patients with a history of convulsive disorders. (Convulsions may possibly occur).
Patients with a history of hypersensitivity to quinolone antibacterial agents.
The elderly. (See "Use in the Elderly as follows.")
Others: Animal studies have shown that Levofloxacin can produce arthropathy in juvenile dogs, young mature dogs (13 months of age) and juvenile rats.
Infusion: In cases of severest pneumococcal pneumonia Levocil may not be the optimal therapy. Hospital acquired infections due to certain pathogens (P. aeruginosa) may require combination therapy.
Infusion Time: The recommended infusion time of at least 60 minutes for Levocil 250 mg (100 ml solution for infusion) should be observed. It is known for ofloxacin, that during infusion tachycardia and a temporary decrease in blood pressure may develop. In rare cases, as a consequence of profound drop in blood pressure, circulatory collapse may occur. If there is a conspicuous drop in blood pressure during infusion of Levofloxacin (l-isomer of ofloxacin), the infusion must be halted immediately.
The risk of getting convulsions during the treatment with Levocil may be increased if in the past brain was damaged for example by a stroke or severe brain injury. Therefore inform the doctor completely about the former diseases. The patient must not be treated with Levocil if they suffer from epilepsy.
The risk of getting convulsions may also be increased by concomitant therapy with fenbufen or comparable nonsteroidal antiphlogistics or with theophylline.
Although photosensitisation (hypersensitivity to light with sunburn-like reactions) is very rare with administration of Levofloxacin, it is recommended that patients should not expose themselves unnecessarily to strong sunlight or to artificial UV rays (e.g. Sunray lamp, solarium), in order to prevent photosensitisation.
The doctor has to be immediately informed if severe, persistent and/or bloody diarrhoea occur during or after treatment with Levocil. It must be stopped immediately and an appropriate therapy must be initiated without delay. Products inhibiting the peristalsis must not be administered in these cases. Tendinitis, rarely observed with quinolones, may occasionally lead to rupture, involving Achilles tendon in particular. Elderly patients are more prone to tendinitis. The risk of tendon rupture may be increased by co-administration of corticosteroids. If tendinitis is suspected, medical advice is to be asked for immediately, treatment with Levocil must be halted, and the affected tendon must be treated approximately, e.g. Immobilization.
Patients with glucose-6 phosphate dehydrogenase deficiency (a hereditary disease) may be prone to destruction of red blood cells (hemolysis) when treated with quinolone antibacterial agents, and so Levofloxacin should be used with caution in these patients.
Some side effects of Levocil like vertigo/dizziness, drowsiness, visual disturbances may impair the ability to concentrate and react. This may constitute a risk in situations where these abilities are of special importance (e.g., Driving a car or operating machinery, working without secure hold). This especially applies to the combination with alcohol.
Use in the Elderly: Tablet: This product is mainly excreted by the kidneys. (See "Pharmacology: Pharmacokinetics under Actions.") Since the elderly often have a renal hypofunction and are in danger of continuous high blood concentration, observe dose and interval (e.g., 100 mg b.i.d.).
Infusion: For elderly patients it is to be considered, that these patients have more often a reduced renal function.
Tablet: Since safety during pregnancy has not been established, this product should not be administered to women who are pregnant or suspected of being pregnant.
Since Levofloxacin is excreted in breast milk, it is recommended that nursing mothers refrain from using this product. If use is necessary, breast feeding should be avoided.
Infusion: Because of missing studies on man and because of the possibility of cartilage damage to growing organisms by quinolones, Levocil must not be administered to pregnant women and during lactation period. If a pregnancy is diagnosed during treatment with Levocil, the doctor has to be informed.
Tablet: Shock: Since shock symptoms may rarely occur, observe patients carefully. If any abnormalities are observed, discontinue the medication and take appropriate measures.
Hypersensitivity: Anaphylactoid symptoms (erythema, chills, dyspnea), edema, urticaria, feeling of warmth or photosensitivity may rarely occur and rash or pruritus may infrequently occur. In the event of such symptoms, discontinue the medication.
Dermatologic: It has been reported that Levofloxacin may rarely cause Lyell Syndrome or Stevens Johnson Syndrome.
Psychoneurologic: Convulsion, tremor or numbness may rarely occur, and insomnia, dizziness or headache may infrequently occur.
Renal: An increase in BUN may frequently occur. It has been reported that Levofloxacin may rarely cause acute renal failure.
Hepatic: an increase in S-GOT, GPT, Al-P or y-GTP or total bilirubin may infrequently occur.
Hematologic: A decrease in leukocytes, erythrocytes, hemoglobin or hematocrit or an increase in eosinophils may infrequently occur. Observe patients carefully, and if any abnormality is observed, discontinue the medication.
Gastro-intestinal: Nausea, vomiting, abdominal discomfort, diarrhea, anorexia, abdominal pain or enlarged feeling of the abdomen may infrequently occur. Since it has been reported that Levofloxacin may rarely cause severe colitis, with blood in the stool, such as pseudomembranous colitis, in the event of abdominal pain or frequent diarrhea take appropriate measures, including immediate discontinuation of the medication.
Muscular: Since rhabdomyolysis with rapid deterioration of renal function characterized by myalgia, weakness, increase in CPK or myoglobin in blood or urine may occur, patients should be cautioned.
Others: 1) Since it has been reported that other new quinolones may rarely cause hypoglycemia (especially in elderly patients with renal disorders), this product should be administered carefully. Malaise may rarely occur.
Infusion: Gastro-intestinal symptoms may occur (gastric or abdominal symptoms, loss of appetite, nausea, vomiting and diarrhoea). The onset of diarrhoea, particularly if severe, persistent and/or bloody during or after treatment with Levocil I.V may less frequently indicate the appearance of pseudomembranous colitis. Suspicion of pseudomembranous colitis requires immediate cessation of administration and treatment with appropriate specific antibiotic therapy. Products inhibiting peristalsis are contraindicated in this clinical situation.
Disturbances of the nervous system e.g. Headache, dizziness, sleep disturbances, unsteady gait and tremor (disturbances of muscular co-ordination), numbness and tingling in the limbs (paraesthesia; visual and auditory disturbances of the senses of taste and smell, hallucinations, convulsions and psychotic reactions such as restlessness, agitation, anxiety, depression and confusion). In some cases these reactions have occurred already after the first dose. In the event of such adverse reactions, Levocil I.V must be discontinued immediately and the doctor informed.
Changes in the blood picture (leukopenia, eosinophilia, neutropenia, agranulocytosis, thrombocytopenia, pancytopenia, haemolytic anaemia), hepatitis and transient increase in liver enzymes and/or bilirubin and in serum creatinine have been observed, interstitial nephritis and acute kidney failure may also occur.
Local irritation, pain and reddening at the injection site, and phlebitis have been observed.
Allergic manifestation may occur in particularly hypersensitivity reactions of the skin such as pruritis, rash, urticaria and vasculitis. Isolated cases of severe bullous eruptions such as Stevens-Johnson syndrome. Toxic epidermal necrolysis (Lyell's syndrome) and erythema exsudativum multiforme have been reported. Photosensitivity reactions (Skin reaction on exposure to strong sunlight and artificial UV rays) have been reported. There have been symptoms such as fever, allergy, pneumonitis, angioedema, hypotension and anaphylactic-like shock. In the event of such reactions, Levocil I.V should be discontinued immediately. Medical treatment (therapy for shock) is imperative.
Tendinitis (eg, Achilles tendon) is less frequently observed with quinolones and if it is suspected, treatment with Levocil I.V should be halted immediately and appropriate treatment (e.g. Immobilization) must be initiated for the affected tendon. Other musculoskeletal side effects such as arthralgia and myalgia have been less frequently observed and less frequent occurrences include: Tendon rupture (Achilles tendon) may occur within 48 hours of starting treatment and may be bilateral.
Muscular weakness which may be of special importance in patients within myasthenia gravis.
Isolated cases of rhabdomyolysis have been reported.
Hypoglycemia, especially in diabetics may occur.
Asthenia, fungal overgrowth and proliferation of other resistant microorganism may occur.
Fluoroquinolones are known to possibly trigger attacks of porphyria in patients suffering with porphyria.
Tablet: Since it has been reported that other quinolones (enoxacin, etc.) used in combination with nonsteroidal anti-inflammatory drugs of phenylacetic/propionic acid derivatives, such as fenbufen, may rarely cause convulsions, this product should be administered carefully.
Since antacids containing aluminium or magnesium and drugs containing iron may interfere with the absorption of Levofloxacin resulting in attenuation of the efficacy of Levofloxacin, it is recommended to refrain from using this product with such products.
Infusion: If the patient takes concomitantly other drugs, ask the doctor or pharmacist, whether they are one of the here mentioned drugs. This also applies to drugs, which were not prescribed by the doctor.
There are indications of a pronounced lowering of the cerebral seizure threshold when quinolones are given concurrently with other agents which lower the seizure threshold (e.g. Theophylline). This also applies to the concomitant administration of quinolones and fenbufen or non-steroidal antiphlogistics (drugs for the treatment of rheumatic diseases).
The elimination of (renal clearance) of Levofloxacin was slightly reduced by cimetidine and probenecid. However, these interactions are unlikely to be of clinical relevance.
Levofloxacin should be given carefully when it is co-administered with drugs that affect a certain mode of elimination (tubular secretion) such as probenecid and cimetidine. This applies especially to patients with impaired renal function.
The half life of cyclosporine was slightly increased when co-administered with levofloxacin.
Instructions: Store below 30°C. Protect from heat, sunlight & moisture.
Infusion: Once the infusion vial has been opened, the infusion solution must be used within three hours stored at 25°C.
The infusion vial can be refrigerated at 2°C to 8°C.
J01MA12 - levofloxacin ; Belongs to the class of fluoroquinolones. Used in the systemic treatment of infections.
Tab 250 mg x 5 x 10's. 500 mg x 10's. Infusion (vial) 500 mg/100 mL x 1's.



 Sign Out
Sign Out