


 Sign Out
Sign Out



In the placebo-controlled trials of 18 to 24 weeks duration, 3,534 patients were included of which 1,183 were treated with placebo and 1.185 with empagliflozin 10mg and 1,166 with empagliflozin 25mg. The overall incidence of adverse events in patients treated with empagliflozin was similar to placebo. The most frequently reported adverse reaction was hypoglycaemia when used with sulphonylurea or insulin (see Description of selected adverse reactions as follows).
Tabulated list of adverse reactions: Adverse reactions classified by system organ class and MedDRA preferred terms reported in patients who received empagliflozin in placebo-controlled studies are presented in the table as follows (Table 11).
The adverse reactions are listed by absolute frequency. Frequencies are defined as very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), or very rare (<1/10,000), and not known (cannot be estimated from the available data). (See Table 11.)
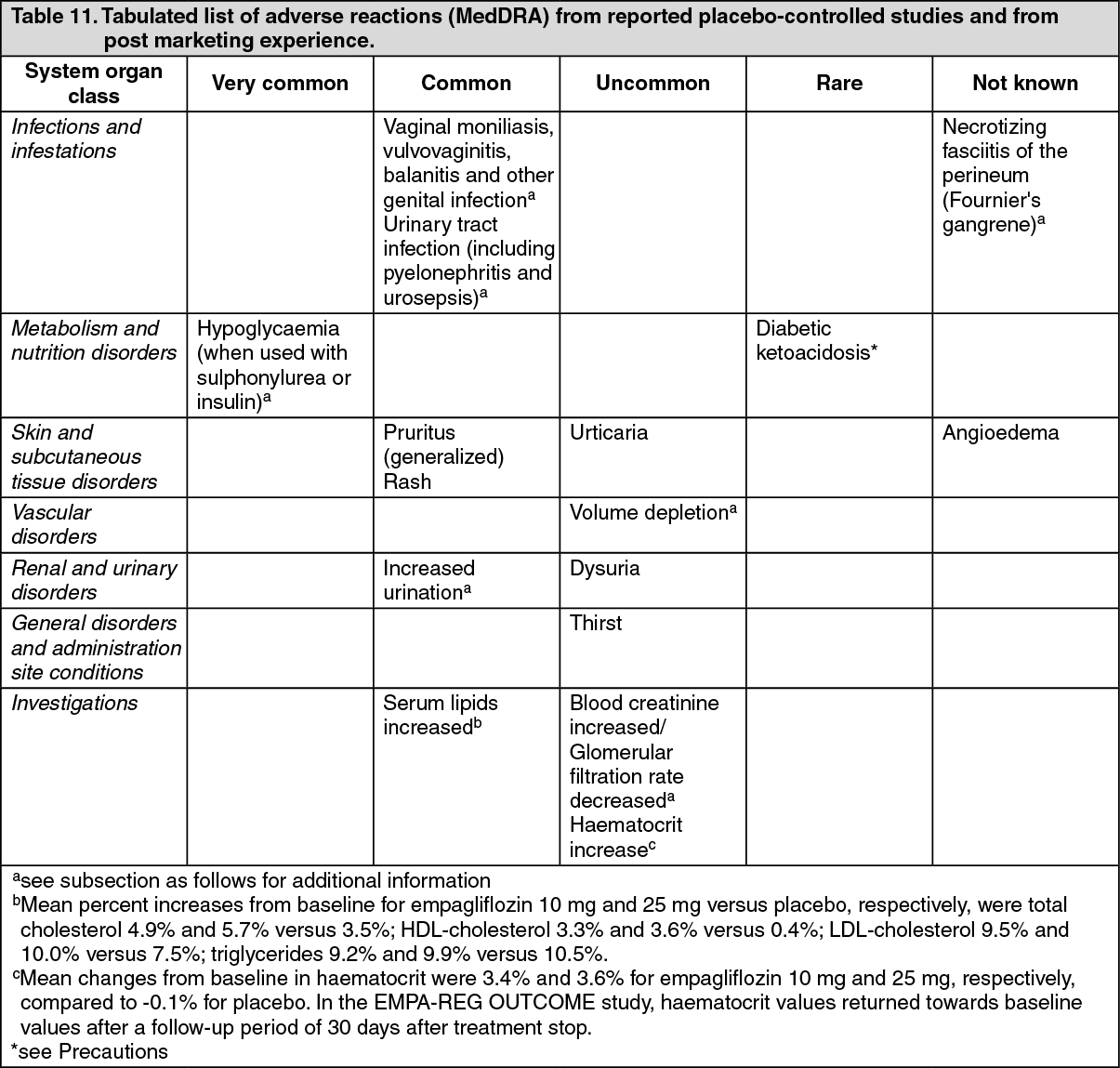 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Hypoglycaemia: The frequency of hypoglycaemia depended on the background therapy in the respective studies and was similar for empagliflozin and placebo as monotherapy, add-on to metformin, add-on to pioglitazone with or without metformin, as add-on to linagliptin and metformin, as adjunct to standard care therapy and for the combination of empagliflozin with metformin in drug-naïve patients compared to those treated with empagliflozin and metformin as individual components and in EMPA-REG OUTCOME study. An increased frequency was noted when given as add-on to metformin and a sulphonylurea (empagliflozin 10 mg: 16.1%, empagliflozin 25 mg: 11.5%, placebo: 8.4%), add-on to basal insulin with or without metformin and with or without a sulphonylurea (empagliflozin 10 mg: 19.5%, empagliflozin 25 mg: 28.4%, placebo: 20.6% during initial 18 weeks treatment when insulin could not be adjusted; empagliflozin 10 mg and 25 mg: 36.1%, placebo 35.3% over the 78-week trial), and add-on to MDI insulin with or without metformin (empagliflozin 10 mg: 39.8%, empagliflozin 25 mg: 41.3%, placebo: 37.2% during initial 18 weeks treatment when insulin could not be adjusted; empagliflozin 10 mg: 51.1%, empagliflozin 25 mg: 57.7%, placebo: 58% over the 52-week trial).
Major hypoglycaemia (event requiring assistance): No increase in major hypoglycaemia was observed with empagliflozin compared to placebo as monotherapy, add-on to metformin, add-on to metformin and a sulphonylurea, and add-on to pioglitazone with or without metformin, add-on to linagliptin and metformin, as adjunct to standard care therapy and for the combination of empagliflozin with metformin in drug-naïve patients compared to those treated with empagliflozin and metformin as individual components. An increased frequency was noted when given as add-on to basal insulin with or without metformin and with or without a sulphonylurea (empagliflozin 10 mg: 0%, empagliflozin 25 mg: 1.3%, placebo: 0% during initial 18 weeks treatment when insulin could not be adjusted; empagliflozin 10 mg: 0%, empagliflozin 25 mg: 1.3%, placebo 0% over the 78-week trial), and add-on to MDI insulin with or without metformin (empagliflozin 10 mg: 0.5 %, empagliflozin 25 mg: 0.5%, placebo: 0.5 % during initial 18 weeks treatment when insulin could not be adjusted; empagliflozin 10 mg: 1.6%, empagliflozin 25 mg: 0.5%, placebo: 1.6% over the 52-week trial). In EMPA-REG OUTCOME study, a slight decreased was observed with empagliflozin compared to placebo (empagliflozin 10mg: 1.4 mg, empagliflozin 25mg: 1.3%, placebo: 1.5%).
Vaginal moniliasis, vulvovaginitis, balanitis and other genital infection: Vaginal moniliasis, vulvovaginitis, balanitis and other genital infections were reported more frequently in patients treated with empagliflozin (empagliflozin 10 mg: 4.0%, empagliflozin 25 mg: 3.9%) compared to placebo (1.0%). These infections were reported more frequently in females treated with empagliflozin compared to placebo, and the difference in frequency was less pronounced in males. The genital tract infections were mild or moderate in intensity.
Increased urination: Increased urination (including the predefined terms pollakiuria, polyuria, and nocturia) was observed at higher frequencies in patients treated with empagliflozin (empagliflozin 10 mg: 3.5%, empagliflozin 25 mg: 3.3%) compared to placebo (1.4%). Increased urination was mostly mild or moderate in intensity. The frequency of reported nocturia was similar for placebo and empagliflozin (<1%).
Urinary tract infection: The overall frequency of urinary tract infection reported as adverse event was similar in patients treated with empagliflozin 25 mg and placebo (7.0% and 7.2%) and higher in empagliflozin 10 mg (8.8%). Similar to placebo, urinary tract infection was reported more frequently for empagliflozin in patients with a history of chronic or recurrent urinary tract infections. The intensity (mild, moderate, severe) of urinary tract infection was similar in patients treated with empagliflozin and placebo. Urinary tract infection was reported more frequently in females treated with empagliflozin compared to placebo; there was no difference in males.
Volume depletion: The overall frequency of volume depletion (including the predefined terms blood pressure (ambulatory) decreased, blood pressure systolic decreased, dehydration, hypotension, hypovolaemia, orthostatic hypotension, and syncope) was similar in patients treated with empagliflozin (empagliflozin 10 mg: 0.6%, empagliflozin 25 mg: 0.4%) and placebo (0.3%). The frequency of volume depletion events was increased in patients 75 years and older treated with empagliflozin 10 mg (2.3%) or empagliflozin 25 mg (4.3%) compared to placebo (2.1%).
Blood creatinine increased/Glomerular filtration rate decreased: The overall frequency of patients with increased blood creatinine and decreased glomerular filtration rate were similar between empagliflozin and placebo (blood creatinine increased: empagliflozin 10mg 0.6%, empagliflozin 25mg 0.1%, placebo 0.5%; glomerular filtration rate decreased: empagliflozin 10mg 0.1%, empagliflozin 25mg 0%, placebo 0.3%).
In placebo-controlled, double-blind studies up to 76 weeks, initial increases in creatinine and initial decreases in estimated glomerular filtration rates in patients treated with empagliflozin were generally transient during continuous treatment or reversible after drug discontinuation of treatment.
View ADR Monitoring Form