Adult: Initially, 0.2 mg (1 mL), followed by subsequent dose of 0.02-1 mg (0.1-5 mL). Subsequent dosage and method of administration depends on the ventricular rate and rapidity with which cardiac pacemaker can take over when the medicine is gradually withdrawn.
Intravenous Adjunct in shock
Adult: 0.5-5 mcg per minute (0.25-2.5 mL of dilution) given via infusion, adjust rate according to patient response.
Adult: Initially, 0.02-0.06 mg (1-3 mL of a 1:50,000 dilution), followed by 0.01-0.2 mg (0.5-10 mL) given via bolus inj. Subsequent dosage and method of administration depends on the ventricular rate and rapidity with which cardiac pacemaker can take over when the medicine is gradually withdrawn. Alternatively, initially, 5 mcg per minute (1.25 mL of a 1:250,000 dilution) given via infusion.
Intravenous Bronchospasm during anaesthesia
Adult: Initially, 0.01-0.02 mg (0.5-1 mL) via bolus inj, may repeat dose if necessary.
Adult: Initially, 0.2 mg (1 mL), followed by subsequent dose of 0.15-0.2 mg (0.75-1 mL). Subsequent dosage and method of administration depends on the ventricular rate and rapidity with which cardiac pacemaker can take over when the medicine is gradually withdrawn.
Reconstitution
IV bolus: Dilute 1 mL of solution labelled as containing 1:5000 solution with 10mL NaCl inj or dextrose 5% inj to make a 1:50,000 solution. IV infusion for heart block; Stokes-Adams attacks; cardiac arrest: Dilute 10 mL of solution labelled as containing 1:5000 solution with 500 mL dextrose 5% inj to make a 1:250,000 solution. IV infusion for shock: Dilute 5 mL of solution labelled as containing 1:5000 solution with 500 mL dextrose 5% inj.
Contraindications
Angina pectoris; ventricular arrhythmias requiring inotropic therapy; tachyarrhythmias; recent MI; tachycardia; heart block due to cardiac glycoside intoxication.
Special Precautions
Patient with CV disease (e.g. coronary artery disease, ischaemic heart disease), hypertension, diabetes mellitus, distributive shock, hyperthyroidism, aneurysms. May exacerbate Adams-Stokes seizures during normal sinus rhythm or transient heart block. Ensure adequate ventilation. Renal and hepatic impairment. Elderly. Pregnancy and lactation.
Adverse Reactions
Cardiac disorders: Tachycardia, palpitations, angina, Stokes-Adams attacks, hypertension, hypotension, ventricular arrhythmias, tachyarrhythmias, pulmonary oedema, dyspnoea. Gastrointestinal disorders: Nausea, vomiting. General disorders and administration site conditions: Sweating, warmth, weakness. Eye disorders: Blurring of vision. Investigations: Increased serum glucose. Metabolism and nutrition disorders: Hypokalaemia. Nervous system disorders: Nervousness, headache, dizziness, restlessness, tension, fear of excitement, tremors. Vascular disorders: Flushing, pallor. Potentially Fatal: Cardiac dysrhythmia and myocardial necrosis.
IM/Inhalation/Respiratory/Intracardiac/IV/Parenteral/PO/SC: C
Patient Counseling Information
This drug may cause dizziness, if affected, do not drive or operate machinery.
Monitoring Parameters
Monitor blood pressure, heart rate, urine flow, ECG, central venous pressure, blood gases. Monitor acid-base balance and correct any electrolyte disturbances.
Overdosage
Symptoms: Tachycardia or other arrhythmias, palpitations, angina, hypotension or hypertension. Management: Supportive and symptomatic treatment. Reduce rate of administration or discontinue isoprenaline. Monitor blood pressure, pulse, respiration, ECG.
Drug Interactions
Enhanced arrhythmogenic effect with inhalational anaesthetics (e.g. halothane and cyclopropane). Antagonistic effects with ß-adrenergic blocking agents (e.g. propranolol, atenolol). Increased risk of cardiac arrhythmias with levodopa. May reduce antianginal effects of nitrates. Magnified effect with MAOIs and chlorpromazine. Potentially Fatal: Severe arrhythmias with epinephrine and digitalis. Additive cardiotoxic properties and potential myocardial necrosis with IV methyl xanthines (e.g. aminophylline and theophylline) and IV corticosteroids.
Action
Description: Isoprenaline is a potent and nonselective ß-adrenergic agonist. It increases heart rate and contractility by its positive inotropic and chronotropic actions. It also relaxes bronchial, gastrointestinal, and uterine smooth muscles. Synonym: Isoproterenol. Onset: Immediate (IV). Duration: 10-15 minutes (IV). Pharmacokinetics: Metabolism: Metabolised in the liver, lungs and other tissues by COMT to major metabolite, 3-O-methylisoprenaline. Excretion: Via urine primarily as sulfate conjugates. Elimination half-life: 2 hours (SC); 2.5-5 minutes (IV).
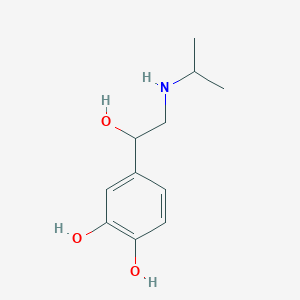
Chemical Structure
Isoprenaline Source: National Center for Biotechnology Information. PubChem Database. Isoprenaline, CID=3779, https://pubchem.ncbi.nlm.nih.gov/compound/Isoprenaline (accessed on Jan. 21, 2020)
R03CB01 - isoprenaline ; Belongs to the class of adrenergics for systemic use, non-selective beta-adrenoreceptor agonists. Used in the treatment of obstructive airway diseases. C01CA02 - isoprenaline ; Belongs to the class of adrenergic and dopaminergic cardiac stimulants excluding glycosides. Used in the treatment of hypotension.
References
Anon. Isoproterenol. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 21/03/2019.Buckingham R (ed). Isoprenaline. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 21/03/2019.Isoproterenol Hydrochloride Injection, Solution (Cipla USA Inc.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 21/03/2019.Pfizer New Zealand Limited. Isuprel Injection data sheet 22 August 2017. Medsafe. http://www.medsafe.govt.nz/. Accessed 21/03/2019.



 Sign Out
Sign Out