Adult: Initially, 250 mg bid for 2 wk, followed by 500-1000 mg daily in divided doses. Max: 1000 mg daily. Adjust dose by monitoring plasma concentrations. Child: 10 mg/kg daily. Adjust doses according to blood concentrations and response.
Renal Impairment
Mild to moderate: Dose reduction may be needed. Severe: Contraindicated.
Administration
May be taken with or without food. May be taken after meals if GI discomfort occurs.
Contraindications
Hypersensitivity. Patient w/ epilepsy, depression, severe anxiety, psychosis, or in those who misuse alcohol. Severe renal impairment.
Special Precautions
Patient w/ porphyria. Mild to moderate renal impairment. Pregnancy and lactation.
Adverse Reactions
Drowsiness, somnolence, dizziness, headache, lethargy, depression, tremor, dysarthria, hyperreflexia, paraesthesia, nervousness, anxiety, vertigo, confusion, disorientation, loss of memory, paresis, major and minor clonic seizures, convulsions, coma; psychosis (possibly w/ suicidal tendencies), personality changes, hyperirritability, aggression; elevated serum aminotransferase levels, esp in patients w/ pre-existing liver disease. Rarely, hypersensitivity reactions including rash, and photosensitivity; cardiac arrhythmias and sudden CHF.
Monitoring Parameters
Monitor renal, hepatic, and hematological functions; plasma cycloserine concentrations.
Overdosage
Symptoms: Headache, vertigo, confusion, drowsiness, hyper-irritability, paraesthesias, dysarthria and psychosis; paresis, convulsions and coma often occur in larger doses. Management: Symptomatic and supportive treatment. Activated charcoal may be more effective than emesis or lavage in reducing absorption. May give 200-300 mg of pyridoxine HCl daily to treat and prevent neurotoxic events. Haemodialysis may remove the drug from the bloodstream but should only be used for life-threatening toxicity.
Drug Interactions
Concomitant use w/ other anti-TB drugs may lead to vit B12 and/or folic acid deficiency, megaloblastic and sideroblastic anaemia. Increased incidence of CNS effects w/ ethionamide and isoniazid. May inhibit hepatic metabolism of phenytoin.
Food Interaction
Alcohol increases risk of epileptic episodes.
Action
Description: Cycloserine inhibits bacterial cell wall synthesis by competing w/ amino acid (D-alanine) for incorporation into the bacterial cell wall. It may be bacteriostatic or bactericidal. Pharmacokinetics: Absorption: Readily and almost completely absorbed from the GI tract. Time to peak plasma concentration: 3-4 hr. Distribution: Widely distributed into body tissues and fluids, including the CSF, placenta, and breast milk. Metabolism: Hepatic. Excretion: Via urine by glomerular filtration (as unchanged drug). Plasma half-life: Approx 10 hr.
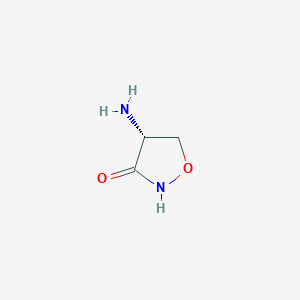
Chemical Structure
Cycloserine Source: National Center for Biotechnology Information. PubChem Database. Cycloserine, CID=6234, https://pubchem.ncbi.nlm.nih.gov/compound/Cycloserine (accessed on Jan. 22, 2020)
Anon. Cycloserine. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 18/08/2014.Buckingham R (ed). Cycloserine. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 18/08/2014.McEvoy GK, Snow EK, Miller J et al (eds). Cycloserine. AHFS Drug Information (AHFS DI) [online]. American Society of Health-System Pharmacists (ASHP). https://www.medicinescomplete.com. Accessed 18/08/2014.Seromycin Capsule (Purdue GMP Center LLC dba The Chao Center). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/. Accessed 18/08/2014.



 Sign Out
Sign Out