


 Sign Out
Sign Out



Pharmacology: Pharmacodynamics: Mechanism of Action: Ivabradine is a pure heart rate-lowering agent, acting by selective and specific inhibition of the cardiac pacemaker If current that controls the spontaneous diastolic depolarisation in the sinus node and regulates heart rate. The cardiac effects are specific to the sinus node with no effect on intra-atrial, atrioventricular or intraventricular conduction times, nor on myocardial contractility or ventricular repolarisation.
Ivabradine can interact also with the retinal current Ih which closely resembles cardiac If. It participates in the temporal resolution of the visual system, by curtailing the retinal response to bright light stimuli. Under triggering circumstances (eg, rapid changes in luminosity), partial inhibition of Ih by ivabradine underlies the luminous phenomena that may be occasionally experienced by patients. Luminous phenomena (phosphenes) are described as a transient enhanced brightness in a limited area of the visual field (see Adverse Reactions).
Pharmacodynamic Effects: The main pharmacodynamic property of ivabradine in humans is a specific dose-dependent reduction in heart rate. Analysis of heart rate reduction with doses up to 20 mg twice daily indicates a trend towards a plateau effect which is consistent with a reduced risk of severe bradycardia <40 beats/min (bpm) (see Adverse Reactions).
At usual recommended doses (5 or 7.5 mg twice daily), heart rate reduction is approximately 10 bpm at rest and during exercise. This leads to a reduction in cardiac workload and myocardial oxygen consumption. Ivabradine does not influence intracardiac conduction, contractility (no negative inotropic effect) or ventricular repolarisation: In clinical electrophysiology studies, ivabradine had no effect on atrioventricular or intraventricular conduction times or corrected QT intervals; in patients with left ventricular dysfunction [left ventricular ejection fraction (LVEF) between 30% and 45%], ivabradine did not have any deleterious influence on LVEF.
Clinical Efficacy and Safety: The antianginal and anti-ischaemic efficacy of Coralan was studied in 5 double-blind randomised trials (3 vs placebo, and 1 each vs atenolol and amlodipine). These trials included a total of 4111 patients with chronic stable angina pectoris, of whom 2617 received ivabradine. Ivabradine 5 mg twice daily was shown to be effective on exercise test parameters within 3-4 weeks of treatment. Efficacy was confirmed with 7.5 mg twice daily. In particular, the additional benefit over 5 mg twice daily was established in a reference-controlled study versus atenolol: Total exercise duration at trough was increased by about 1 min after 1 month of treatment with 5 mg twice daily and further improved by almost 25 sec after an additional 3-month period with forced titration to 7.5 mg twice daily. In this study, the antianginal and anti-ischaemic benefits of ivabradine were confirmed in patients ≥65 years. The efficacy of 5 and 7.5 mg twice daily was consistent across studies on exercise test parameters (total exercise duration, time to limiting angina, time to angina onset and time to 1 mm ST segment depression) and was associated with a decrease of about 70% in the rate of angina attacks. The twice-daily dosing regimen of ivabradine gave uniform efficacy over 24 hrs.
In 889-patient randomised placebo-controlled study, ivabradine given on top of atenolol 50 mg once daily showed additional efficacy on all ETT parameters at the trough of drug activity (12 hrs after oral intake).
In 725-patient randomised placebo-controlled study, ivabradine did not show additional efficacy on top of amlodipine at the trough of ivabradine activity (12 hrs after oral intake) while an additional efficacy was shown at peak (3-4 hrs after oral intake).
Ivabradine efficacy was fully maintained throughout the 3- or 4-month treatment periods in the efficacy trials. There was no evidence of pharmacological tolerance (loss of efficacy) developing during treatment nor of rebound phenomena after abrupt treatment discontinuation. The antianginal and anti-ischaemic effects of ivabradine were associated with dose-dependent reductions in heart rate and with a significant decrease in rate pressure product (heart rate x systolic blood pressure) at rest and during exercise. The effects on blood pressure and peripheral vascular resistance were minor and not clinically significant.
A sustained reduction of heart rate was demonstrated in patients treated with ivabradine for at least 1 year (n=713). No influence on glucose or lipid metabolism was observed.
The antianginal and anti-ischaemic efficacy of ivabradine was preserved in diabetic patients (n=457) with a similar safety profile as compared to the overall population.
A large outcome study, BEAUTIFUL, was performed in 10,917 patients with coronary artery disease and left ventricular dysfunction (LVEF <40%) on top of optimal background therapy with 86.9% of patients receiving β-blockers. The main efficacy criterion was the composite of cardiovascular death, hospitalization for acute myocardial infarction (MI) or hospitalization for new onset or worsening heart failure. The study showed no difference in the rate of the primary composite outcome in the ivabradine group by comparison to the placebo group (relative risk ivabradine:placebo 1, p=0.945).
In a post-hoc subgroup of patients with symptomatic angina at randomisation (n=1507), no safety signal was identified regarding cardiovascular death, hospitalization for acute MI or heart failure (ivabradine 12% vs placebo 15.5%, p=0.05).
A large outcome study, SHIFT, was performed in 6505 adult patients with moderate to severe symptoms of chronic heart failure (CHF), with a reduced left ventricular ejection fraction (LVEF ≤35%).
The SHIFT study was a multicentre, international, randomised double-blind placebo controlled trial. The trial population presented a systolic CHF with NYHA class II to IV and in stable condition for ≥4 weeks, with documented hospital admission for worsening HF within 12 months before selection, in sinus rhythm at selection with resting heart rate ≥70 bpm. Patients received standard care including β-blockers (89%), ACE inhibitors and/or angiotensin II antagonists (91%), diuretics (83%) and anti-aldosterone agents (60%). In the ivabradine group, 67% of patients were treated with 7.5 mg twice a day. The median follow-up duration was 22.9 months.
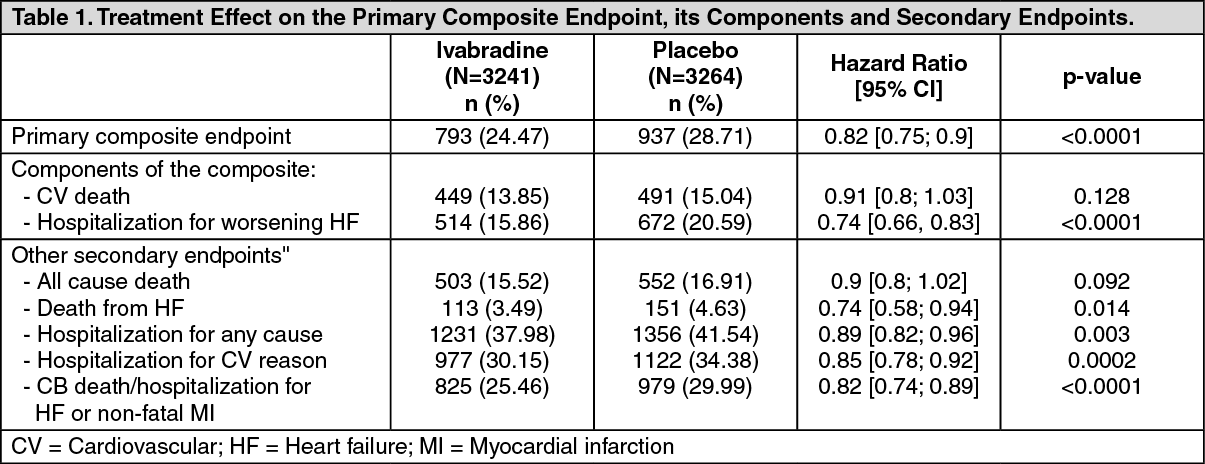
The primary endpoint was a composite of cardiovascular mortality and hospitalisation for worsening heart failure. The study demonstrated a clinically and statistically significant relative risk reduction of 18% in the rate of the primary composite endpoint [hazard ratio ivabradine; placebo: 0.82, 95%CI (0.75;0.9) - p<0.0001]. The absolute risk reduction was 4.2%. The treatment effect was apparent within 3 months of initiation of treatment.
The reduction in the primary endpoint was observed consistently irrespective of age, gender, NYHA class, β-blocker treatment or not, ischaemic or non-ischaemic heart failure aetiology and of background history of diabetes or hypertension.
Treatment of ivabradine for 1 year would prevent 1 cardiovascular death or hospital admission for heart failure for every 26 patients treated. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThere was a significant improvement in NYHA class at last recorded value, 887 (28%) of patients on ivabradine improved versus 776 (24%) of patients on placebo (p=0.001).
Treatment with ivabradine was associated with an average reduction in heart rate of 15 bpm from a baseline value of 80 bpm, which was maintained throughout the course of study.
Pharmacokinetics: Under physiological conditions, ivabradine is rapidly released from tablets and is highly water-soluble (>10 mg/mL). Ivabradine is the S-enantiomer with no bioconversion demonstrated in vivo. The N-desmethylated derivative of ivabradine has been identified as the main active metabolite in humans.
Absorption and Bioavailability: Ivabradine is rapidly and almost completely absorbed after oral administration with a peak plasma level reached in about 1 hr under fasting condition. The absolute bioavailability of the film-coated tablets is around 40%, due to first-pass effect in the gut and liver. Food delayed absorption by approximately 1 hr and increased plasma exposure by 20-30%. The intake of the tablet during meals is recommended in order to decrease intraindividual variability in exposure (see Dosage & Administration).
Distribution: Ivabradine is approximately 70% plasma protein bound and the volume of distribution at steady state is close to 100 L in patients. The maximum plasma concentration following chronic administration at the recommended dose of 5 mg twice daily is 22 ng/mL (CV=29%). The average plasma concentration is 10 ng/mL (CV=38%) at steady state.
Biotransformation: Ivabradine is extensively metabolised by the liver and the gut by oxidation through cytochrome P-450 3A4 (CYP3A4) only. The major active metabolite is the N-desmethylated derivative (S 18982) with an exposure about 40% of that of the parent compound. The metabolism of this active metabolite also involves CYP3A4. Ivabradine has low affinity for CYP3A4, shows no clinically relevant CYP3A4 induction or inhibition and is therefore unlikely to modify CYP3A4 substrate metabolism or plasma concentrations. Inversely, potent inhibitors and inducers may substantially affect ivabradine plasma concentrations (see Interactions).
Elimination: Ivabradine is eliminated with a main half-life of 2 hrs (70-75% of the AUC) in plasma and an effective half-life of 11 hrs. The total clearance is about 400 mL/min and the renal clearance is about 70 mL/min. Excretion of metabolites occurs to a similar extent via faeces and urine. About 4% of an oral dose is excreted unchanged in urine.
Linearity/Nonlinearity: The kinetics of ivabradine is linear over an oral dose range of 0.5-24 mg.
Special Populations: Elderly: No pharmacokinetic differences (AUC and Cmax) have been observed between elderly (≥65 years) or very elderly patients (≥75 years) and the overall population (see Dosage & Administration).
Renal Insufficiency: The impact of renal impairment (creatinine clearance from 15-60 mL/min) on ivabradine pharmacokinetic is minimal, in relation with the low contribution of renal clearance (about 20%) to total elimination for both ivabradine and its main metabolite S 18982 (see Dosage & Administration).
Hepatic Impairment: In patients with mild hepatic impairment (Child-Pugh score up to 7) unbound AUC of ivabradine and the main active metabolite were about 20% higher than in subjects with normal hepatic function. Data are insufficient to draw conclusions in patients with moderate hepatic impairment. No data are available in patients with severe hepatic impairment (see Dosage & Administration and Contraindications).
Pharmacokinetic/Pharmacodynamic (PK/PD) Relationship: PK/PD relationship analysis has shown that heart rate decreases almost linearly with increasing ivabradine and S 18982 plasma concentrations for doses of up to 15-20 mg twice daily. At higher doses, the decrease in heart rate is no longer proportional to ivabradine plasma concentrations and tends to reach a plateau. High exposures to ivabradine that may occur when ivabradine is given in combination with strong CYP3A4 inhibitors may result in an excessive decrease in heart rate although this risk is reduced with moderate CYP3A4 inhibitors (see Contraindications, Warnings, Precautions and Interactions).
Toxicology: Preclinical Safety Data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential. Reproductive toxicity studies showed no effect of ivabradine on fertility in male and female rats. When pregnant animals were treated during organogenesis at exposures close to therapeutic doses, there was a higher incidence of foetuses with cardiac defects in the rat and a small number of foetuses with ectrodactylia in the rabbit.
In dogs given ivabradine (doses of 2, 7 or 24 mg/kg/day) for 1 year, reversible changes in retinal function were observed but were not associated with any damage to ocular structures. These data are consistent with the pharmacological effect of ivabradine related to its interaction with hyperpolarisation-activated Ih currents in the retina, which share extensive homology with the cardiac pacemaker If current.
Other long-term repeat dose and carcinogenicity studies revealed no clinically relevant changes.