Oral Prophylaxis of venous thromboembolic events following hip replacement surgery, Prophylaxis of venous thromboembolic events following knee replacement surgery
Adult: 2.5 mg bid, starting 12-24 hours after surgery. Duration of treatment: 10-14 days (knee replacement); 32-38 days (hip replacement). Refer to detailed product guidelines when transitioning between anticoagulants.
Oral Prophylaxis of stroke and systemic embolism in non-valvular atrial fibrillation
Adult: In patients with ≥1 risk factor e.g. prior stroke or TIA, age ≥75 years, hypertension, diabetes mellitus, symptomatic heart failure (NYHA Class ≥II): 5 mg bid. Refer to detailed product guidelines when transitioning between anticoagulants. Elderly: Refer to the Special Patient Group section.
Oral Deep vein thrombosis, Pulmonary embolism
Adult: Treatment: 10 mg bid for 7 days followed by 5 mg bid. Prophylaxis of recurrent cases: 2.5 mg bid following completion of ≥6 months of anticoagulant treatment. Refer to detailed product guidelines when transitioning between anticoagulants.
Special Patient Group
Patients taking strong CYP3A4 and P-gp inhibitors (e.g. itraconazole, ketoconazole, voriconazole, posaconazole, ritonavir): Reduce dose by 50% if taking doses of 5 mg or 10 mg bid. If already taking 2.5 mg bid, avoid co-administration of apixaban.
Prophylaxis of stroke and systemic embolism in non-valvular atrial fibrillation:
Dose reduction in patients with at least 2 of the following criteria: ≥80 years old, body weight ≤60 kg, serum creatinine ≥1.5 mg/dL (133 micromole/L): 2.5 mg bid.
Patients undergoing cardioversion: 5 mg bid for at least 2.5 days (5 single doses) prior to procedure. For patients meeting the criteria for dose reduction: 2.5 mg bid for at least 2.5 days (5 single doses). If cardioversion is required before the completion of 5 single doses, administer a 10 mg loading dose at least 2 hours before cardioversion, followed by 5 mg bid. For patients meeting the criteria for dose reduction: 5 mg loading dose at least 2 hours before cardioversion, followed by 2.5 mg bid.
Renal Impairment
Patients undergoing dialysis: Not recommended.
Prophylaxis of venous thromboembolic events following knee replacement surgery; Prophylaxis of venous thromboembolic events following hip replacement surgery; Deep vein thrombosis; Pulmonary embolism:
CrCl (mL/min)
Dosage
<15
Not recommended.
Prophylaxis of stroke and systemic embolism in non-valvular atrial fibrillation:
Mild to moderate: Refer to the Special Patient Group section.
CrCl (mL/min)
Dosage
<15
Not recommended.
15-29
2.5 mg bid.
Hepatic Impairment
Severe (Child-Pugh class C): Not recommended.
Administration
May be taken with or without food.
Contraindications
Active pathological bleeding, hepatic disease associated with coagulopathy and clinically relevant bleeding risk, lesions or conditions with significant risk factors for major bleeding (e.g. current or recent gastrointestinal ulceration, malignant neoplasms at high risk of bleeding, recent intracranial haemorrhage; recent brain or spinal injury; recent brain, spinal or ophthalmic surgery; known or suspected oesophageal varices; arteriovenous malformations, vascular aneurysms or major intraspinal or intracerebral vascular abnormalities). Concomitant use with other anticoagulants (e.g. unfractionated heparin [UFH], LMWH, oral anticoagulants) except under specific circumstances of switching anticoagulant therapy, or when UFH is given at doses necessary to maintain an open central venous or arterial catheter, or when UFH is given during catheter ablation for atrial fibrillation.
Special Precautions
Patient with increased risk of haemorrhage, active cancer, body weight ≤60 kg. Not recommended for patients with prosthetic heart valves or with triple-positive antiphospholipid syndrome (APS). Not recommended as an alternative to UFH for the initial treatment of patients with pulmonary embolism who are haemodynamically unstable or who may receive thrombolysis or pulmonary embolectomy. Patients undergoing cardioversion, elective surgery or invasive procedures, or those who are receiving neuraxial anaesthesia or undergoing spinal puncture. Premature discontinuation increases the risk of thrombotic events; consider alternative anticoagulant treatment if apixaban is discontinued for a reason other than pathological bleeding or completion of a course of therapy. Renal and severe hepatic impairment. Elderly. Pregnancy and lactation. Patients taking strong CYP3A4 and P-gp inhibitors/inducers.
Adverse Reactions
Blood and lymphatic system disorders: Anaemia, thrombocytopenia. Eye disorders: Eye haemorrhage, including conjunctival haemorrhage. Gastrointestinal disorders: Nausea, gastrointestinal or rectal haemorrhage, gingival bleeding. Injury, poisoning and procedural complications: Contusion. Investigations: Increased gamma-glutamyltransferase. Renal and urinary disorders: Haematuria. Respiratory, thoracic and mediastinal disorders: Epistaxis. Vascular disorders: Haemorrhage, haematoma, hypotension (including procedural hypotension). Potentially Fatal: Severe haemorrhage.
Monitor CBC, aPTT, prothrombin time, serum creatinine, and liver function prior to initiation, when clinically indicated, and at least annually thereafter. Observe closely for signs and symptoms of blood loss.
Overdosage
Symptoms: Haemorrhagic complications. Management: Initiate appropriate treatment (e.g. surgical haemostasis, transfusion of fresh frozen plasma, administration of a reversal agent for factor Xa inhibitors). Activated charcoal may be administered within 2-6 hours of ingestion. For life-threatening situations or uncontrolled bleeding, prothrombin complex concentrates (PCCs) or recombinant factor VIIa may be administered.
Drug Interactions
Concomitant use of drugs affecting haemostasis (e.g. aspirin and other antiplatelet agents, SSRIs, serotonin-norepinephrine reuptake inhibitors, NSAIDs) may increase the risk of bleeding. May increase plasma concentration with strong CYP3A4 and P-gp inhibitors (e.g. itraconazole, ketoconazole, voriconazole, posaconazole, ritonavir). May decrease plasma concentration with strong CYP3A4 and P-gp inducers (e.g. rifampicin, phenytoin, carbamazepine, phenobarbital). Potentially Fatal: Concomitant use with other anticoagulant agents, including UFH, LMWHs (e.g. enoxaparin, dalteparin), heparin derivatives (e.g. fondaparinux), oral anticoagulants (e.g. warfarin, rivaroxaban, dabigatran) increased the risk of bleeding.
Food Interaction
Decreased plasma concentration with St. John's wort.
Action
Description: Apixaban is a direct, highly selective and reversible active site inhibitor of free and clot-bound factor Xa (FXa). FXa plays a central role in the blood coagulation cascade by serving as the convergence point for the intrinsic and extrinsic pathways. Inhibition of FXa prevents the conversion of prothrombin to thrombin thereby reducing thrombin generation and thrombus development. Onset: 3-4 hours. Pharmacokinetics: Absorption: Rapidly absorbed from the gastrointestinal tract. Bioavailability: Approx 50%. Time to peak plasma concentration: 3-4 hours. Distribution: Volume of distribution: Approx 21 L. Plasma protein binding: Approx 87%. Metabolism: Metabolised in the liver mainly via O-demethylation and hydroxylation at the 3-oxopiperidinyl moiety by the CYP3A4 and CYP3A5 isoenzymes, and to a lesser extent by CYP1A2, CYP2C8, CYP2C9, CYP2C19, and CYP2J2 isoenzymes. Excretion: Via urine (approx 27% as unchanged drug); faeces. Elimination half-life: Approx 12 hours.
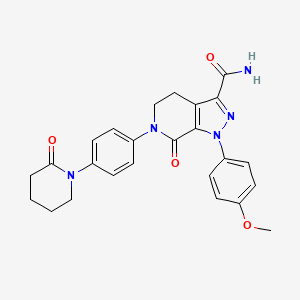
Chemical Structure
Apixaban Source: National Center for Biotechnology Information. PubChem Compound Summary for CID 10182969, Apixaban. https://pubchem.ncbi.nlm.nih.gov/compound/10182969. Accessed July 28, 2022.
Storage
Store between 15-30°C. Storage recommendations may vary among countries or individual products (refer to detailed product guidelines).
B01AF02 - apixaban ; Belongs to the class of direct factor Xa inhibitors. Used in the treatment of thrombosis.
References
Anon. Apixaban. AHFS Clinical Drug Information [online]. Bethesda, MD. American Society of Health-System Pharmacists, Inc. https://www.ahfscdi.com. Accessed 16/06/2022.Anon. Apixaban. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 16/06/2022.Apixaban 5 mg Film-coated Tablets (Teva UK Limited). MHRA. https://products.mhra.gov.uk. Accessed 16/06/2022.Apixaban Tablet, Film Coated (Indoco Remedies Limited). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed. Accessed 16/06/2022.Buckingham R (ed). Apixaban. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 16/06/2022.Eliquis 2.5 mg Film-coated Tablets (Bristol-Myers Squibb/Pfizer EEIG). MHRA. https://products.mhra.gov.uk. Accessed 16/06/2022.Eliquis Film Coated Tablets 2.5 mg, 5 mg (Pfizer Malaysia Sdn. Bhd.). National Pharmaceutical Regulatory Agency - Ministry of Health Malaysia. https://www.npra.gov.my. Accessed 16/06/2022.Eliquis Tablet, Film Coated; Eliquis 30-Day Starter Pack (E.R. Squibb & Sons, L.L.C.). DailyMed. Source: U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed. Accessed 16/06/2022.Joint Formulary Committee. Apixaban. British National Formulary [online]. London. BMJ Group and Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 16/06/2022.Pfizer New Zealand Limited. Eliquis 2.5 mg and 5 mg Film-coated Tablets data sheet 30 August 2019. Medsafe. http://www.medsafe.govt.nz. Accessed 16/06/2022.



 Sign Out
Sign Out