Adult: Initially, 1 mg daily, increased to 5-15 mg daily in 3-4 divided doses. Elderly: May require lower doses.
Oral Parkinsonism
Adult: Initially, 1 mg daily, gradually increased at intervals of 3-5 days by increments of 2 mg until 6-10 mg daily in 3-4 divided doses. Postencephalitic patients: Up to 12-15 mg daily. Elderly: May require lower doses.
Administration
Should be taken with food. Best taken w/ meals. Take before meals if dry mouth occurs, after meals if drooling/nausea occurs. Take at the same time each day.
Special Precautions
Patient w/ arteriosclerosis, history of drug idiosyncrasy. CV disease, glaucoma, GI obstruction, prostatic hyperplasia and/or urinary stricture. Not intended for treatment of tardive dyskinesia. Avoid abrupt withdrawal. Hepatic and renal impairment. Elderly. Pregnancy and lactation.
Adverse Reactions
Dryness of the mouth, nausea, constipation, vomiting, dizziness, drowsiness, headache, blurred vision, mydriasis, nervousness, tachycardia, urinary hesitancy or retention, increased intraocular tension, angle-closure glaucoma, weakness, rashes, dilatation of the colon, paralytic ileus, and suppurative parotitis. Rarely, psychiatric disturbances (e.g. delusion, amnesia, depersonalization, sense of unreality, paranoia).
May impair mental or physical abilities e.g. operating machinery or driving.
Monitoring Parameters
Perform gonioscopic examination prior to initiation of therapy. Monitor intraocular pressure at regular intervals during prolonged treatment.
Overdosage
Symptoms: Flushing, dryness of the skin, dilated pupils, dry mouth and tongue, tachycardia, rapid respiration, hyperpyrexia, HTN, nausea, vomiting, rashes on face or upper trunk; restlessness, confusion, hallucinations, paranoid and psychotic reactions, incoordination, delirium and occasionally convulsions; CNS depression may occur w/ coma, circulatory and resp failure, death. Management: Symptomatic and supportive treatment. Maintain adequate airway. Admin diazepam to control excitement and convulsions but consider risk of CNS depression. Hypoxia and acidosis should be corrected.
Drug Interactions
Increased antimuscarinic side effects w/ phenothiazines, clozapine, antihistamines, disopyramide, nefopam and amantadine. Synergistic effect when concomitantly used w/ TCAs. Concurrent admin w/ MAOIs may cause dry mouth, blurred vision, urinary hesitancy or retention and constipation. May antagonise effect of metoclopramide and domperidone on GI function. Reduced absorption of levodopa. May antagonise effect of parasympathomimetics.
Food Interaction
Sedative effects may be potentiated w/ alcohol.
Action
Description: Mechanism of Action: Trihexyphenidyl HCl is a tertiary amine antimuscarinic which exerts a direct inhibitory effect on the parasympathetic nervous system. It also exhibits a direct spasmolytic action on smooth muscle, weak mydriatic, antisialagogue and cardiovagal blocking effects. Onset: W/in 1 hr. Duration: 6-12 hr. Pharmacokinetics: Absorption: Rapidly and well absorbed from the GI tract. Time to peak plasma concentration: 1.3 hr. Metabolism: Undergoes hydroxylation of the alicyclic group. Excretion: Via urine (as unchanged drug) and bile. Elimination half-life: 33 hr.
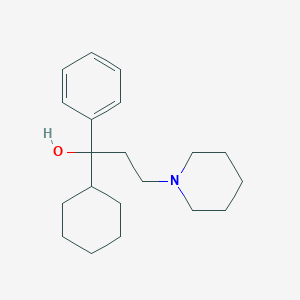
Chemical Structure
Trihexyphenidyl Source: National Center for Biotechnology Information. PubChem Database. Trihexyphenidyl, CID=5572, https://pubchem.ncbi.nlm.nih.gov/compound/Trihexyphenidyl (accessed on Jan. 23, 2020)
Anon. Trihexyphenidyl. Lexicomp Online. Hudson, Ohio. Wolters Kluwer Clinical Drug Information, Inc. https://online.lexi.com. Accessed 04/09/2014.Buckingham R (ed). Trihexyphenidyl Hydrochloride. Martindale: The Complete Drug Reference [online]. London. Pharmaceutical Press. https://www.medicinescomplete.com. Accessed 04/09/2014.McEvoy GK, Snow EK, Miller J et al (eds). Trihexyphenidyl Hydrochloride. AHFS Drug Information (AHFS DI) [online]. American Society of Health-System Pharmacists (ASHP). https://www.medicinescomplete.com. Accessed 04/09/2014.



 Sign Out
Sign Out